

Characterization of Electrograms from Multipolar Diagnostic Catheters during Atrial Fibrillation
- PMID: 26581316
- PMCID: PMC4637153
- DOI: 10.1155/2015/272954
Characterization of Electrograms from Multipolar Diagnostic Catheters during Atrial Fibrillation
Abstract
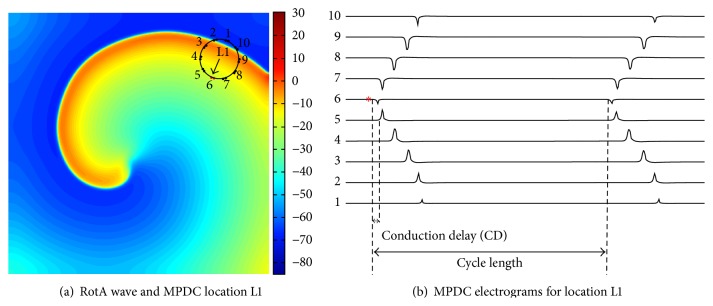
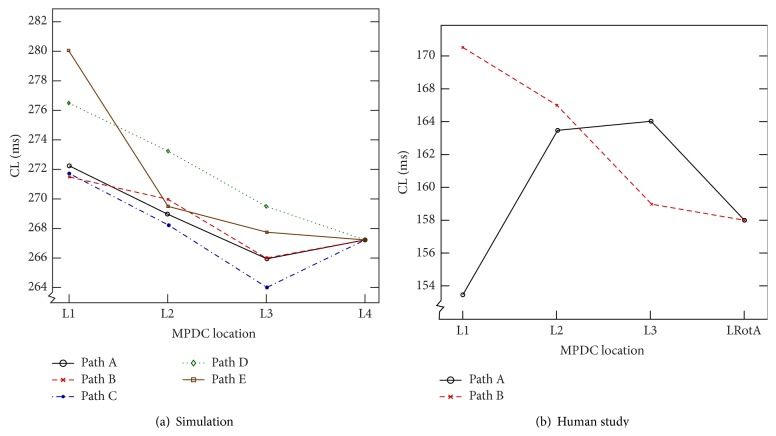
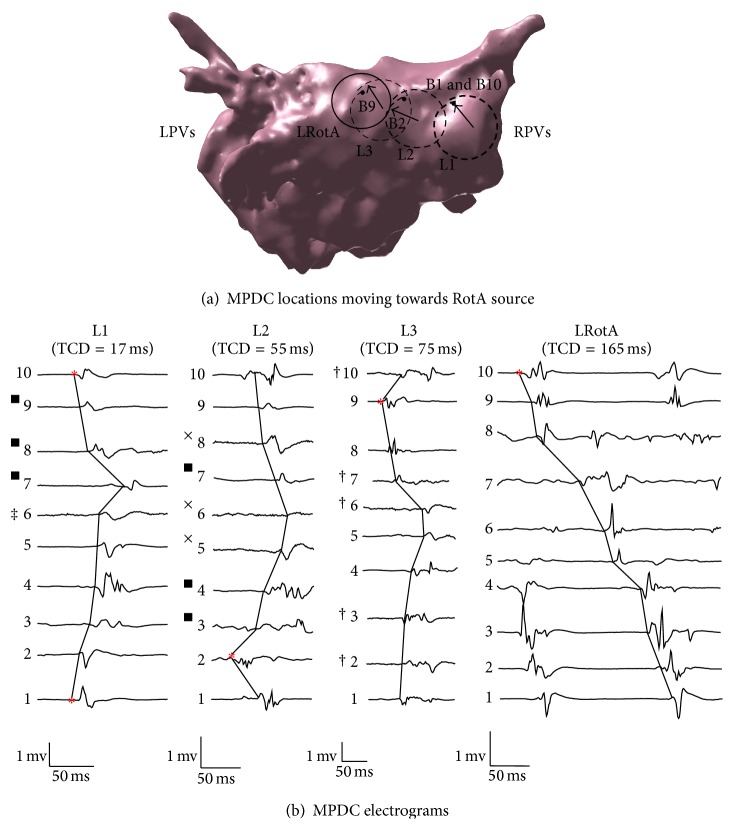
Atrial fibrillation (AF) is the most common arrhythmia in USA with more than 2.3 million people affected annually. Catheter ablation procedure is a method for treatment of AF, which involves 3D electroanatomic mapping of the patient's left atrium (LA) by maneuvering a conventional multipolar diagnostic catheter (MPDC) along the LA endocardial surface after which pulmonary vein (PV) isolation is performed, thus eliminating the AF triggers originating from the PVs. However, it remains unclear how to effectively utilize the information provided by the MPDC to locate the AF-sustaining sites, known as sustained rotor-like activities (RotAs). In this study, we use computer modeling to investigate the variations in the characteristics of the MPDC electrograms, namely, total conduction delay (TCD) and average cycle length (CL), as the MPDC moves towards a RotA source. Subsequently, a study with a human subject was performed in order to verify the predictions of the simulation study. The conclusions from this study may be used to iteratively direct an MPDC towards RotA sources thus allowing the RotAs to be localized for customized and improved AF ablation.
Figures




References
-
- Jalife J., Berenfeld O., Skanes A., Mandapati R. Mechanisms of atrial fibrillation: mother rotors or multiple daughter wavelets, or both? Journal of Cardiovascular Electrophysiology. 1998;9(8, supplement):S2–S12. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
