

Patterns and predictors of failure following tri-modality therapy for locally advanced esophageal cancer
- PMID: 26581671
- PMCID: PMC6854665
- DOI: 10.3109/0284186X.2015.1110252
Patterns and predictors of failure following tri-modality therapy for locally advanced esophageal cancer
Abstract
Background: Although tri-modality therapy is an acceptable standard of care in patients with locally advanced esophageal cancer, data regarding patterns of failure is lacking. We report bi-institutional patterns of failure experience treating patients using tri-modality therapy.
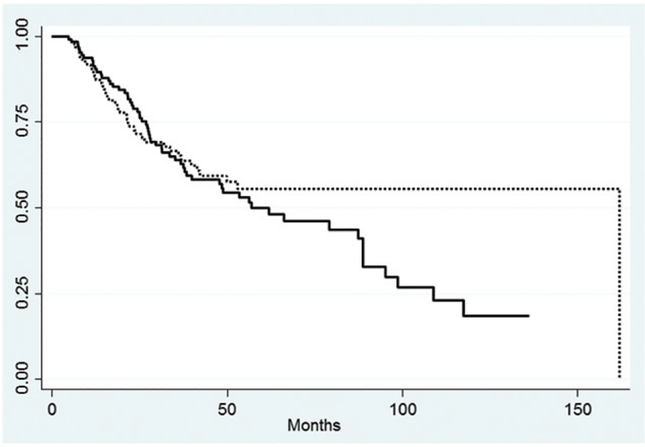
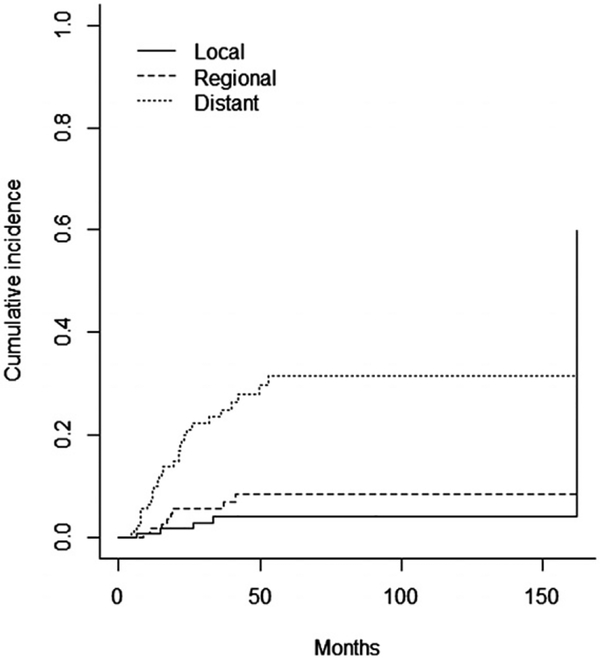
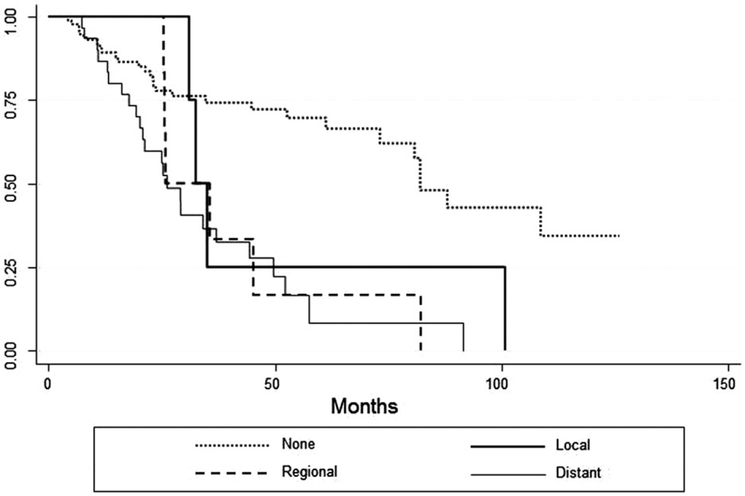
Materials and methods: We retrospectively reviewed patients who underwent chemoradiation followed by esophagectomy between 2006 and 2011 at two NCI-designated cancer centers. First failure sites were categorized as local, regional nodal, or distant. Statistical analysis was performed using Fisher's exact test, non-parametric Wilcoxon rank-sum test, and multiple logistic regression. Kaplan-Meier curves were generated for relapse-free survival (RFS) and overall survival.
Results: A total of 132 patients met the inclusion criteria with a median age of 62 (range 36-80) and median follow-up of 28 months (range 4-128). There were a total of six (4.5%) local, 13 (10%) regional nodal, and 32 (23.5%) distant failures. Local failure was correlated with fewer lymph nodes (LN) assessed (p = 0.01) and close/positive margins (p < 0.01). Regional nodal failure was correlated with fewer LN assessed (p < 0.01) and larger pretreatment tumor size (p = 0.04). Patients with ≤13 LN evaluated had an inferior locoregional RFS versus patients with >13 LN evaluated (p = 0.003). Distant recurrence was correlated with higher pathologic nodal stage (p < 0.001), ulceration (p = 0.017), perineural invasion (p = 0.029), residual disease (p = 0.004), and higher post-treatment PET SUV max (p = 0.049). Patients with a pathologic complete response (OR 0.19, 95% CI 0.05-0.68) were less likely to experience distant recurrence.
Conclusion: Tumor and treatment factors may predict for failure in patients undergoing tri-modality therapy for locally advanced esophageal cancer. Further data is needed to identify patterns of failure in these patients.
Conflict of interest statement
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Figures
References
-
- Ajani JA, D’Amico TA, Almhanna K, Bentrem DJ, Besh S, Chao J, et al. Esophageal and esophagogastric junction cancers, version 1.2015. J Natl Compr Canc Netw. 2015;13:194–227. - PubMed
-
- van Hagen P, Hulshof MC, van Lanschot JJ, Steyerberg EW, van Berge Henegouwen MI, Wijnhoven BP, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. New England J Med. 2012;366:2074–84. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA: Cancer J Clin. 2015;65:5–29. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous