

Effect of Lymph Node Count on Pathological Stage III Rectal Cancer with Preoperative Radiotherapy
- PMID: 26582242
- PMCID: PMC4652213
- DOI: 10.1038/srep16990
Effect of Lymph Node Count on Pathological Stage III Rectal Cancer with Preoperative Radiotherapy
Abstract
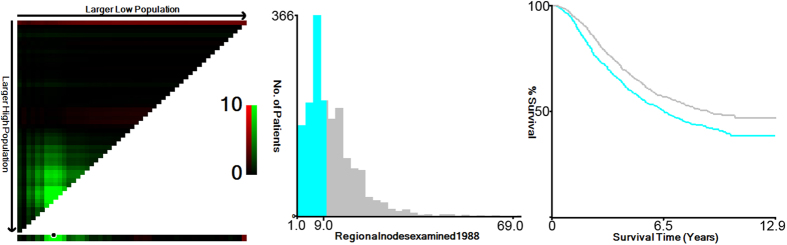
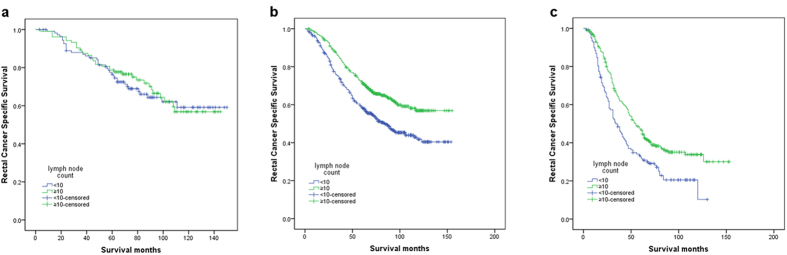
Lymph node (LN) status after surgery for rectal cancer is affected by preoperative radiotherapy. The purpose of this study was to perform a population-based evaluation of the impact of pathologic LN status after neoadjuvant radiotherapy on survival. A total of 1,650 patients receiving neoadjuvant chemotherapy in Surveillance, Epidemiology, and End Results Program (SEER)-registered ypIII stage rectal cancer was analyzed. We identified the optimal cutoff for retrieved LNs as 10 (χ2 = 14.006, P < 0.001), which was validated as an independent prognosis factors in a Cox regression model. Further analysis showed that the LN count was only a prognosis factor with the number from 8 to 16(except for 13).After the number 16, the 5-year survival rate decreased gradually. Collectively, our results confirmed that the number of LNs in yp III stage rectal patients was a prognosis factor only with the numbers from 8 to 16(except for 13). Using the total mesorectal excision technique with an adequate pathologic examination, a large number of LNs retrieved (≥17) might indicate worse tumor response grade and poorer survival.
Figures
References
-
- Kapiteijn E. et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med 345, 638–646 (2001). - PubMed
-
- Sauer R. et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med 351, 1731–1740 (2004). - PubMed
-
- Hong K. D., Lee S. I. & Moon H. Y. Lymph node ratio as determined by the 7th edition of the American Joint Committee on Cancer staging system predicts survival in stage III colon cancer. J Surg Oncol 103, 406–410 (2011). - PubMed
-
- Suzuki O. et al. Number of lymph node metastases is better predictor of prognosis than level of lymph node metastasis in patients with node-positive colon cancer. J Am Coll Surg 202, 732–736 (2006). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
