

Can knowledge-based DVH predictions be used for automated, individualized quality assurance of radiotherapy treatment plans?
- PMID: 26584574
- PMCID: PMC4653923
- DOI: 10.1186/s13014-015-0542-1
Can knowledge-based DVH predictions be used for automated, individualized quality assurance of radiotherapy treatment plans?
Abstract
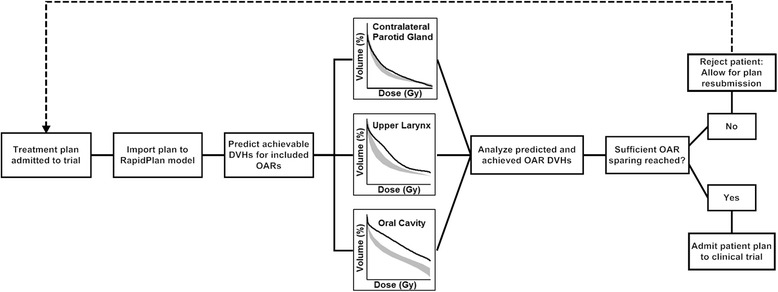
Background: Treatment plan quality assurance (QA) is important for clinical studies and for institutions aiming to generate near-optimal individualized treatment plans. However, determining how good a given plan is for that particular patient (individualized patient/plan QA, in contrast to running through a checklist of generic QA parameters applied to all patients) is difficult, time consuming and operator-dependent. We therefore evaluated the potential of RapidPlan, a commercial knowledge-based planning solution, to automate this process, by predicting achievable OAR doses for individual patients based on a model library consisting of historical plans with a range of organ-at-risk (OAR) to planning target volume (PTV) geometries and dosimetries.
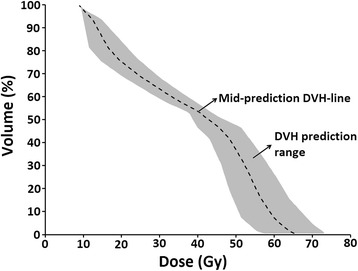
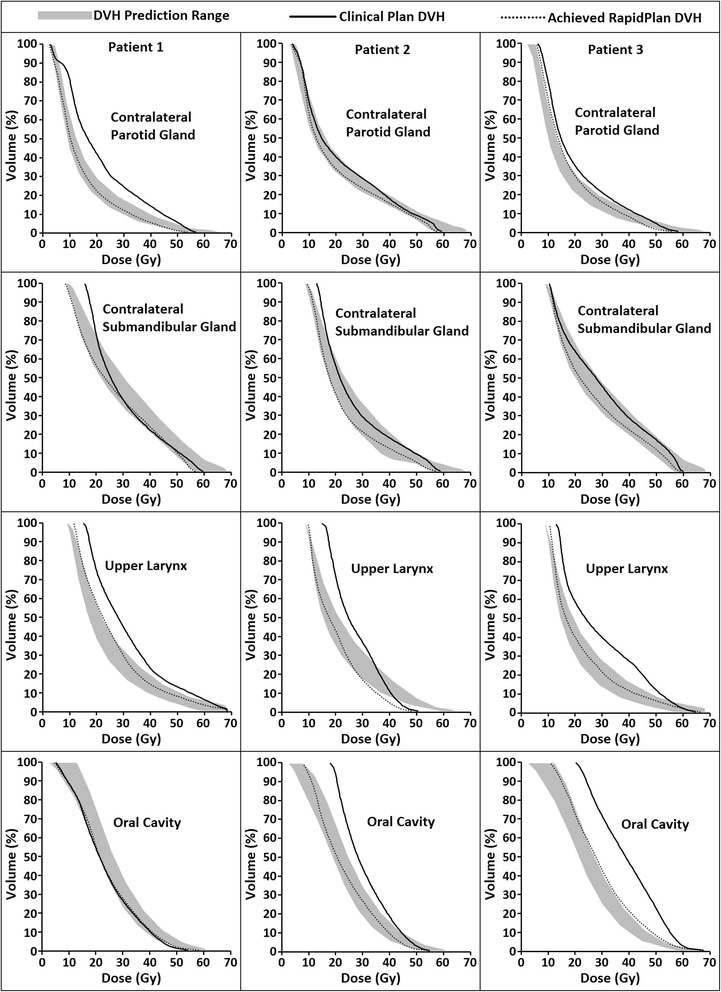
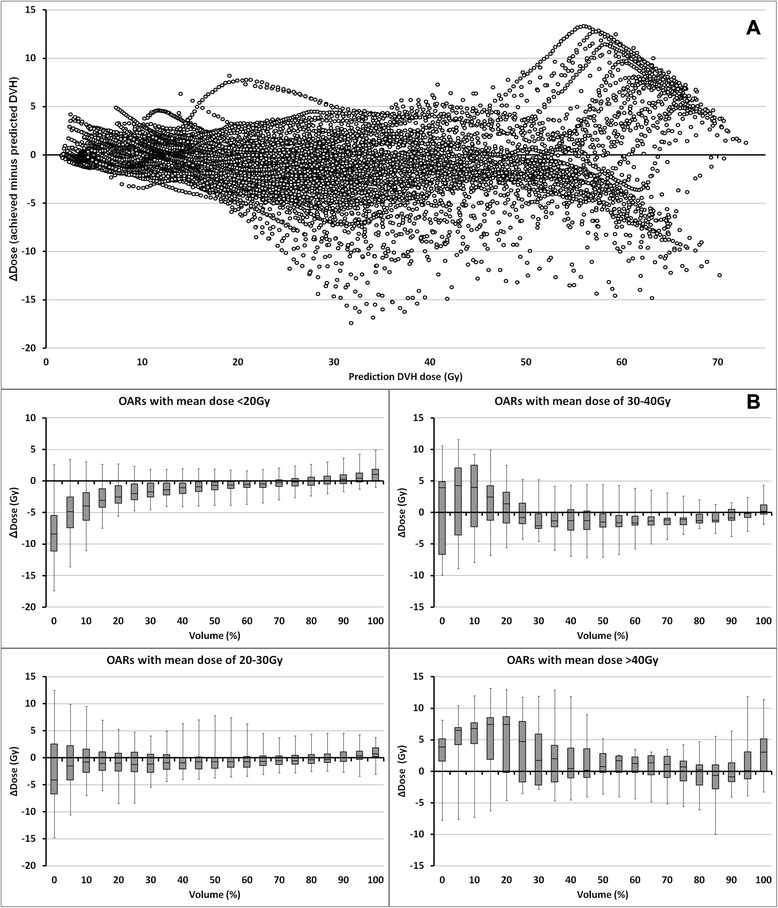
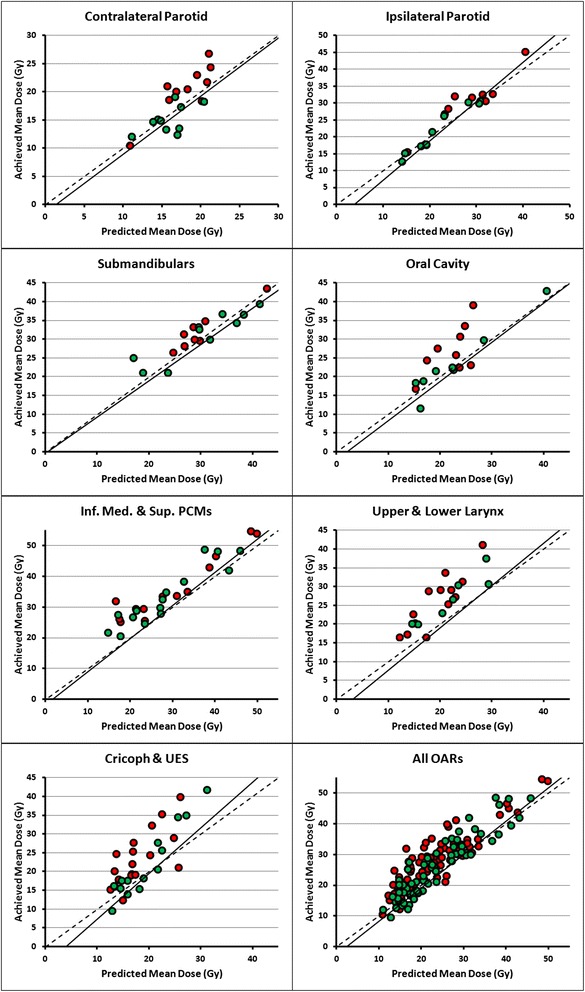
Methods: A 90-plan RapidPlan model, generated using previously created automatic interactively optimized (AIO) plans, was used to predict achievable OAR dose-volume histograms (DVHs) for the parotid glands, submandibular glands, individual swallowing muscles and oral cavities of 20 head and neck cancer (HNC) patients using a volumetric modulated (RapidArc) simultaneous integrated boost technique. Predicted mean OAR doses were compared with mean doses achieved when RapidPlan was used to make a new plan. Differences between the achieved and predicted DVH-lines were analyzed. Finally, RapidPlan predictions were used to evaluate achieved OAR sparing of AIO and manual interactively optimized plans.
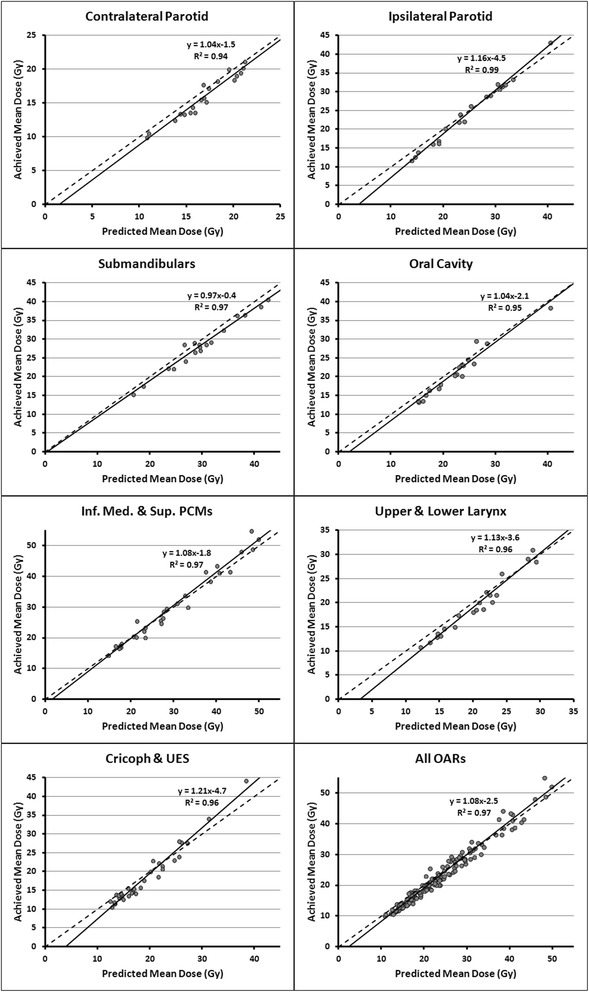
Results: For all OARs, strong linear correlations (R(2) = 0.94-0.99) were found between predicted and achieved mean doses. RapidPlan generally overestimated the amount of achievable sparing for OARs with a large degree of OAR-PTV overlap. RapidPlan QA using predicted doses alone identified that for 50 % (10/20) of the manually optimized plans, sparing of the composite salivary glands, oral cavity or composite swallowing muscles could be improved by at least 3 Gy, 5 Gy or 7 Gy, respectively, while this was the case for 20 % (4/20) AIO plans. These predicted gains were validated by replanning the identified patients using RapidPlan.
Conclusions: Strong correlations between predicted and achieved mean doses indicate that RapidPlan could accurately predict achievable mean doses. This shows the feasibility of using RapidPlan DVH prediction alone for automated individualized head and neck plan QA. This has applications in individual centers and clinical trials.
Figures



References
-
- Das IJ, Cheng C-W, Chopra KL, Mitra RK, Srivastava SP, Glatstein E. Intensity-modulated radiation therapy dose prescription, recording, and delivery: patterns of variability among institutions and treatment planning systems. J Natl Cancer Inst. 2008;100:300–7. doi: 10.1093/jnci/djn020. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
