

Hyperoxia in intensive care, emergency, and peri-operative medicine: Dr. Jekyll or Mr. Hyde? A 2015 update
- PMID: 26585328
- PMCID: PMC4653126
- DOI: 10.1186/s13613-015-0084-6
Hyperoxia in intensive care, emergency, and peri-operative medicine: Dr. Jekyll or Mr. Hyde? A 2015 update
Abstract
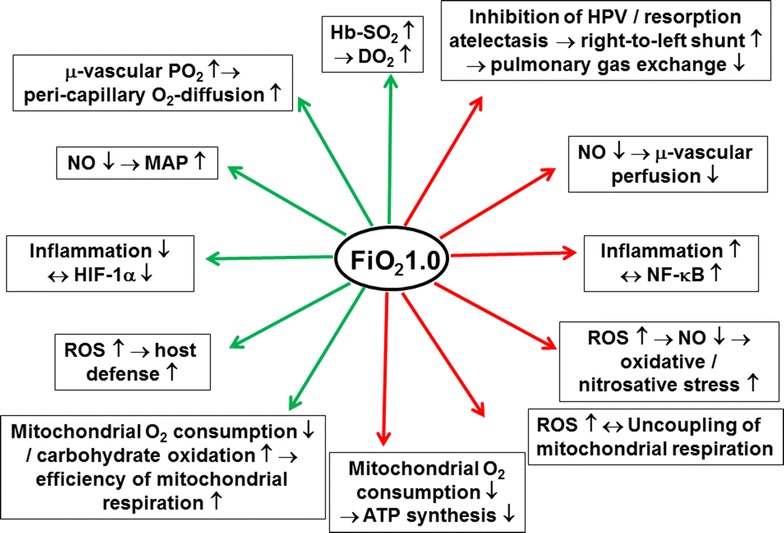
This review summarizes the (patho)-physiological effects of ventilation with high FiO2 (0.8-1.0), with a special focus on the most recent clinical evidence on its use for the management of circulatory shock and during medical emergencies. Hyperoxia is a cornerstone of the acute management of circulatory shock, a concept which is based on compelling experimental evidence that compensating the imbalance between O2 supply and requirements (i.e., the oxygen dept) is crucial for survival, at least after trauma. On the other hand, "oxygen toxicity" due to the increased formation of reactive oxygen species limits its use, because it may cause serious deleterious side effects, especially in conditions of ischemia/reperfusion. While these effects are particularly pronounced during long-term administration, i.e., beyond 12-24 h, several retrospective studies suggest that even hyperoxemia of shorter duration is also associated with increased mortality and morbidity. In fact, albeit the clinical evidence from prospective studies is surprisingly scarce, a recent meta-analysis suggests that hyperoxia is associated with increased mortality at least in patients after cardiac arrest, stroke, and traumatic brain injury. Most of these data, however, originate from heterogenous, observational studies with inconsistent results, and therefore, there is a need for the results from the large scale, randomized, controlled clinical trials on the use of hyperoxia, which can be anticipated within the next 2-3 years. Consequently, until then, "conservative" O2 therapy, i.e., targeting an arterial hemoglobin O2 saturation of 88-95 % as suggested by the guidelines of the ARDS Network and the Surviving Sepsis Campaign, represents the treatment of choice to avoid exposure to both hypoxemia and excess hyperoxemia.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
