

Physician versus non-physician delivery of alcohol screening, brief intervention and referral to treatment in adult primary care: the ADVISe cluster randomized controlled implementation trial
- PMID: 26585638
- PMCID: PMC4653951
- DOI: 10.1186/s13722-015-0047-0
Physician versus non-physician delivery of alcohol screening, brief intervention and referral to treatment in adult primary care: the ADVISe cluster randomized controlled implementation trial
Abstract
Background: Unhealthy alcohol use is a major contributor to the global burden of disease and injury. The US Preventive Services Task Force has recommended alcohol screening and intervention in general medical settings since 2004. Yet less than one in six US adults report health care professionals discussing alcohol with them. Little is known about methods for increasing implementation; different staffing models may be related to implementation effectiveness. This implementation trial compared delivery of alcohol screening, brief intervention and referral to specialty treatment (SBIRT) by physicians versus non-physician providers receiving training, technical assistance, and feedback reports.
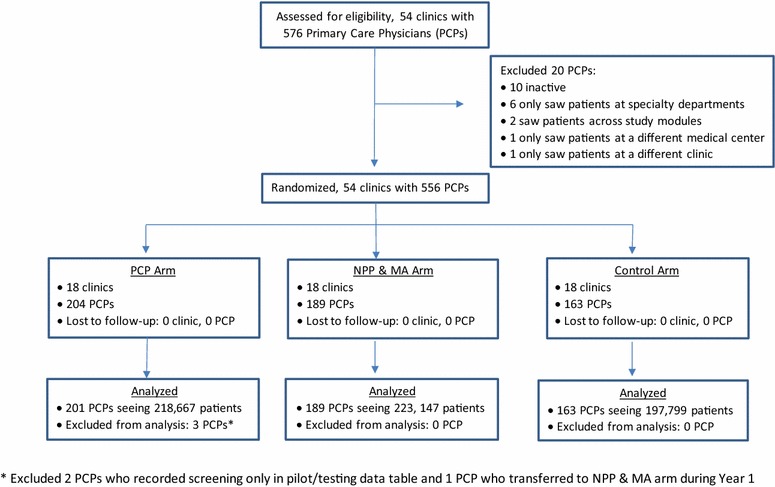
Methods: The study was a cluster randomized implementation trial (ADVISe [Alcohol Drinking as a Vital Sign]). Within a private, integrated health care system, 54 adult primary care clinics were stratified by medical center and randomly assigned in blocked groups of three to SBIRT by physicians (PCP arm) versus non-physician providers and medical assistants (NPP and MA arm), versus usual care (Control arm). NIH-recommended screening questions were added to the electronic health record (EHR) to facilitate SBIRT. We examined screening and brief intervention and referral rates by arm. We also examined patient-, physician-, and system-level factors affecting screening rates and, among those who screened positive, rates of brief intervention and referral to treatment.
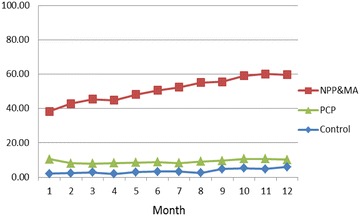
Results: Screening rates were highest in the NPP and MA arm (51 %); followed by the PCP arm (9 %) and the Control arm (3.5 %). Screening increased over the 12 months after training in the NPP and MA arm but remained stable in the PCP arm. The PCP arm had higher brief intervention and referral rates (44 %) among patients screening positive than either the NPP and MA arm (3.4 %) or the Control arm (2.7 %). Higher ratio of MAs to physicians was related to higher screening rates in the NPP and MA arm and longer appointment times to screening and intervention rates in the PCP arm.
Conclusion: Findings suggest that time frames longer than 12 months may be required for full SBIRT implementation. Screening by MAs with intervention and referral by physicians as needed can be a feasible model for increasing the implementation of this critical and under-utilized preventive health service within currently predominant primary care models.
Trial registration: Clinical Trials NCT01135654.
Figures
References
-
- US Department of Health and Human Services, National Institute on Alcohol Abuse and Alcoholism. 10th special report to the US Congress on alcohol and health : highlights from current research from the Secretary of Health and Human Services. Rockville, MD: US Department of Health and Human Services. June 2000. http://pubs.niaaa.nih.gov/publications/10Report/10thSpecialReport.pdf. Accessed 8 Oct 2015.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
