

Nonselective carotid artery ultrasound screening in patients undergoing coronary artery bypass grafting: Is it necessary?
- PMID: 26586360
- PMCID: PMC5125380
- DOI: 10.1016/j.jtcvs.2015.09.108
Nonselective carotid artery ultrasound screening in patients undergoing coronary artery bypass grafting: Is it necessary?
Abstract
Objectives: To determine whether nonselective preoperative carotid artery ultrasound screening alters management of patients scheduled for coronary artery bypass grafting (CABG), and whether such screening affects neurologic outcomes.
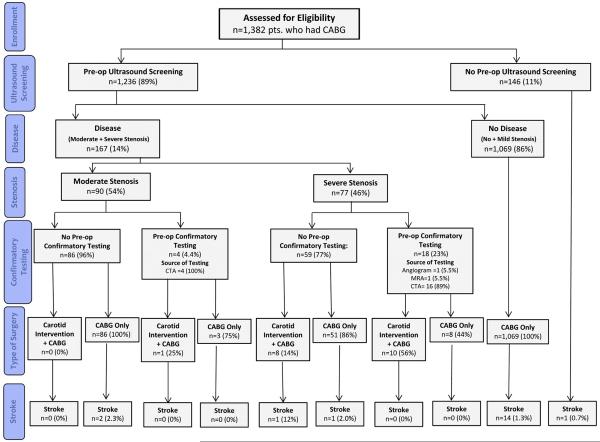
Methods: From March 2011 to September 2013, preoperative carotid artery ultrasound screening was performed on 1236 of 1382 patients (89%) scheduled to undergo CABG. Carotid artery stenosis (CAS) was classified as none or mild (any type 0%-59% stenosis), moderate (unilateral 60%-79% stenosis), or severe (bilateral 60%-79% stenosis or unilateral 80%-100% stenosis).
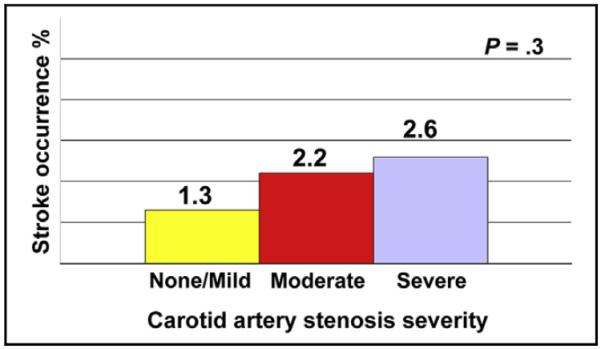
Results: A total of 1069 (86%) had <moderate; 90 (7.3%) had moderate; and 77 (6.2%) had severe CAS. Of those with moderate CAS, 4 (4.4%) had preoperative confirmatory testing, and 1 (1.1%) underwent combined CABG + carotid endarterectomy (CEA); 11 (12%) had off-pump surgery. Of those with severe CAS, 18 (23%) had confirmatory testing, and 18 (23%) underwent combined CABG + CEA; 6 (7.8%) had off-pump surgery. Stroke occurred in 14 of 1069 (1.3%) patients with <moderate CAS; 2 of 90 (2.2%) of those with moderate CAS; and 2 of 77 (2.6%) of those with severe CAS (P = .3). In patients with ≥moderate CAS, 1 of 19 (5.3%) undergoing CABG + CEA and 3 of 148 (2.0%) undergoing CABG alone experienced stroke (P = .4). In patients with moderate CAS, stroke occurred in 1 of 11 (9.1%) off-pump and 1 of 79 (1.3%) on-pump patients (P = .2). In patients with severe CAS, stroke occurred in 1 of 6 (17%) off-pump and 1 of 71 (1.4%) on-pump patients (P = .15).
Conclusions: Routine preoperative carotid artery evaluation altered the management of a minority of patients undergoing CABG; this did not translate into perioperative stroke risk. Hence, a more targeted approach for preoperative carotid artery evaluation should be adopted.
Keywords: carotid endarterectomy; carotid stenosis; coronary artery bypass grafting; ultrasound screening.
Copyright © 2016 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Discussion.J Thorac Cardiovasc Surg. 2016 Feb;151(2):408-9. doi: 10.1016/j.jtcvs.2015.09.114. Epub 2015 Nov 14. J Thorac Cardiovasc Surg. 2016. PMID: 26586356 No abstract available.
-
Preoperative carotid ultrasound through the looking glass: Curiouser and curiouser!J Thorac Cardiovasc Surg. 2016 Feb;151(2):410-1. doi: 10.1016/j.jtcvs.2015.10.079. Epub 2015 Oct 28. J Thorac Cardiovasc Surg. 2016. PMID: 26589537 No abstract available.
References
-
- Tarakji KG, Sabik JF, III, Bhudia SK, Batizy LH, Blackstone EH. Temporal onset, risk factors, and outcomes associated with stroke after coronary artery bypass grafting. JAMA. 2011;305:381–90. - PubMed
-
- Fukuda I, Gomi S, Watanabe K, Seita J. Carotid and aortic screening for coronary artery bypass grafting. Ann Thorac Surg. 2000;70:2034–9. - PubMed
-
- Anastasiadis K, Karamitsos TD, Velissaris I, Makrygiannakis K, Kiskinis D. Preoperative screening and management of carotid artery disease in patients undergoing cardiac surgery. Perfusion. 2009;24:257–62. - PubMed
-
- Durand DJ, Perler BA, Roseborough GS, Grega MA, Borowicz LM, Jr, Baumgartner WA, et al. Mandatory versus selective preoperative carotid screening: a retrospective analysis. Ann Thorac Surg. 2004;78:159–66. discussion 166. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
