

Hepatic Shock Differential Diagnosis and Risk Factors: A Review Article
- PMID: 26587034
- PMCID: PMC4644574
- DOI: 10.5812/hepatmon.27063
Hepatic Shock Differential Diagnosis and Risk Factors: A Review Article
Abstract
Context: Liver as an important organ has a vital role in physiological processes in the body. Different causes can disrupt normal function of liver. Factors such as hypo-perfusion, hypoxemia, infections and some others can cause hepatic injury and hepatic shock.
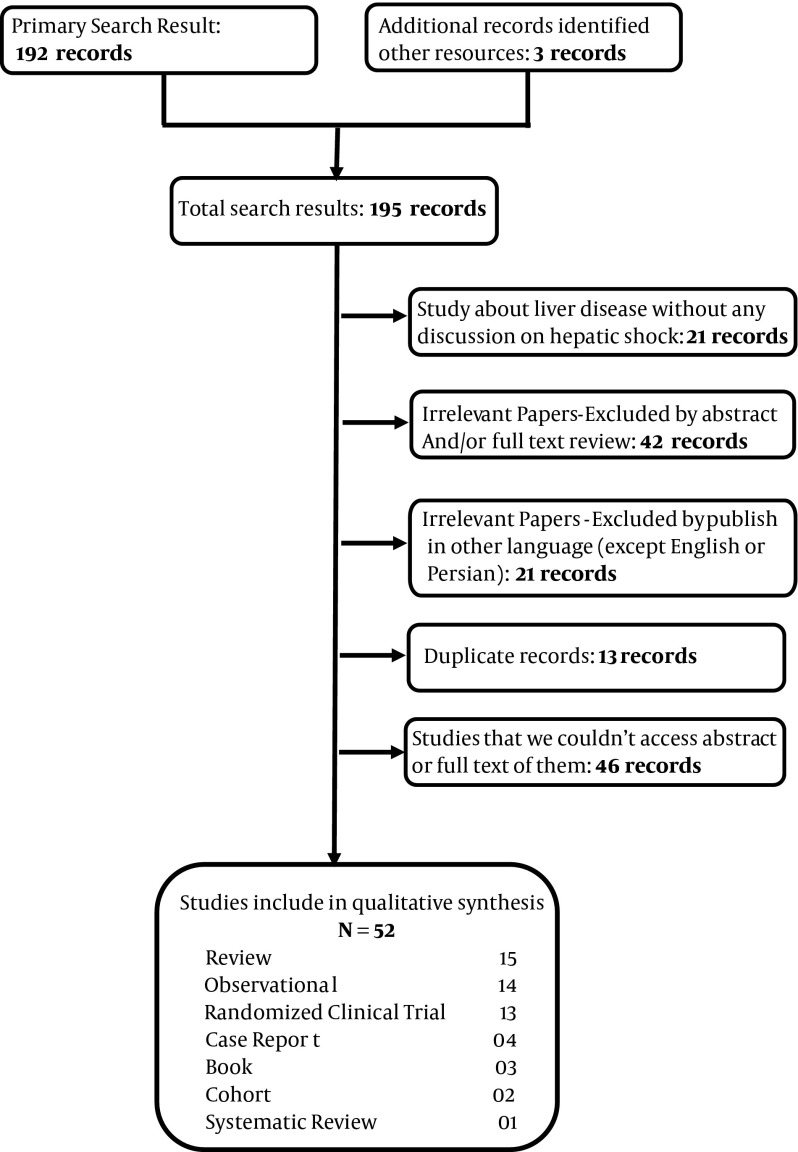
Evidence acquisition: Published research resources from 2002 to May 2015 in some databases (PubMed, Scopus, Index Copernicus, DOAJ, EBSCO-CINAHL, Science direct, Cochrane library and Google scholar and Iranian search database like SID and Iranmedex) were investigated for the present study.
Results: Different causes can lead to hepatic shock. Most of these causes can be prevented by early resuscitation and treatment of underlying factors.
Conclusions: Hepatic shock is detected in ill patients, especially those with hemodynamic disorders. It can be prevented by early treatment of underlying disease. There is no definite treatment for hepatic shock and should be managed conservatively. Hepatic shock in patients can increase the mortality rate.
Keywords: Hepatitis; Injury; Liver; Shock.
Similar articles
-
Hepatic Alveolar Hydatid Cyst: A Brief Review of Published Cases from Iran in the Last 20 Years.Hepat Mon. 2016 Sep 11;16(10):e38920. doi: 10.5812/hepatmon.38920. eCollection 2016 Oct. Hepat Mon. 2016. PMID: 27882065 Free PMC article. Review.
-
Food Reduction in Avicenna's View and Related Principles in Classical Medicine.Iran Red Crescent Med J. 2016 May 24;18(6):e25760. doi: 10.5812/ircmj.25760. eCollection 2016 Jun. Iran Red Crescent Med J. 2016. PMID: 27621927 Free PMC article. Review.
-
Hepatotoxicity of halogenated inhalational anesthetics.Iran Red Crescent Med J. 2014 Sep 5;16(9):e20153. doi: 10.5812/ircmj.20153. eCollection 2014 Sep. Iran Red Crescent Med J. 2014. PMID: 25593732 Free PMC article. Review.
-
The prevalence of tuberculosis among Iranian elderly patients admitted to the infectious ward of hospital: A systematic review and meta-analysis.Int J Mycobacteriol. 2016 Dec;5 Suppl 1:S199-S200. doi: 10.1016/j.ijmyco.2016.11.022. Epub 2016 Nov 27. Int J Mycobacteriol. 2016. PMID: 28043551
-
Melatonin receptors mediate improvements of liver function but not of hepatic perfusion and integrity after hemorrhagic shock in rats.Crit Care Med. 2008 Jan;36(1):24-9. doi: 10.1097/01.CCM.0000292088.33318.F0. Crit Care Med. 2008. PMID: 18090374
Cited by
-
The Pivotal Role of Presepsin in Assessing Sepsis-Induced Cholestasis.Diagnostics (Basel). 2024 Aug 6;14(16):1706. doi: 10.3390/diagnostics14161706. Diagnostics (Basel). 2024. PMID: 39202194 Free PMC article.
-
Pseudohypoadrenalism, a subclinical cortisol metabolism disorder in hyperuricemia.Front Endocrinol (Lausanne). 2023 Nov 16;14:1279205. doi: 10.3389/fendo.2023.1279205. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 38034015 Free PMC article.
-
Myxedema Coma Complicated by Pancytopenia.Case Rep Med. 2019 Jul 14;2019:2320751. doi: 10.1155/2019/2320751. eCollection 2019. Case Rep Med. 2019. PMID: 31396281 Free PMC article.
-
[Diagnosing acute organ ischemia : A practical guide for the emergency and intensive care physician].Med Klin Intensivmed Notfmed. 2020 Mar;115(2):159-172. doi: 10.1007/s00063-020-00655-6. Epub 2020 Feb 21. Med Klin Intensivmed Notfmed. 2020. PMID: 32086542 German.
-
Pathophysiological Changes During Ischemia-reperfusion Injury in Rodent Hepatic Steatosis.In Vivo. 2020 May-Jun;34(3):953-964. doi: 10.21873/invivo.11863. In Vivo. 2020. PMID: 32354880 Free PMC article. Review.
References
-
- Seeto RK, Fenn B, Rockey DC. Ischemic hepatitis: clinical presentation and pathogenesis. Am J Med. 2000;109(2):109–13. - PubMed
-
- Emmanuel A, Inns S. Ischemic/Hypoxic Hepititis. Lecture Notes: Gastroenterology and Hepatology. Oxford: Willey-Blackwell; 2002. pp. 1024–100.
-
- Soultati A, Dourakis SP. Liver dysfunction in the intensive care unit. Ann Gastroenterol. 2007;18(1):35–45.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources