

The Assessment of Addition of Either Intravenous Paracetamol or Diclofenac Suppositories to Patient-Controlled Morphine Analgesia for Postgastrectomy Pain Control
- PMID: 26587407
- PMCID: PMC4644315
- DOI: 10.5812/aapm.29688
The Assessment of Addition of Either Intravenous Paracetamol or Diclofenac Suppositories to Patient-Controlled Morphine Analgesia for Postgastrectomy Pain Control
Abstract
Background: Major surgical procedures, such as gastrectomy, result in extensive postoperative pain, which can lead to increased morbidity, discomfort and dissatisfaction among the patients.
Objectives: The aim of this study was to evaluate the effect of adding diclofenac suppositories or intravenous paracetamol, on morphine consumption and on the quality of postgastrectomy pain control.
Patients and methods: This randomized double blinded clinical trial was carried out in 90 patients with gastric cancer, who were candidates for gastrectomy, which were divided into three similar groups. The patients were transferred to an intensive care unit after the operation and received patient-controlled analgesia (PCA) with morphine, morphine PCA plus intravenous paracetamol 1 g, every 6 hours, and morphine PCA plus diclofenac suppositories, 100 mg every 8 hours. The patients were evaluated for up to 24 hours after the operation for the severity of pain, alertness, and opioid complications.
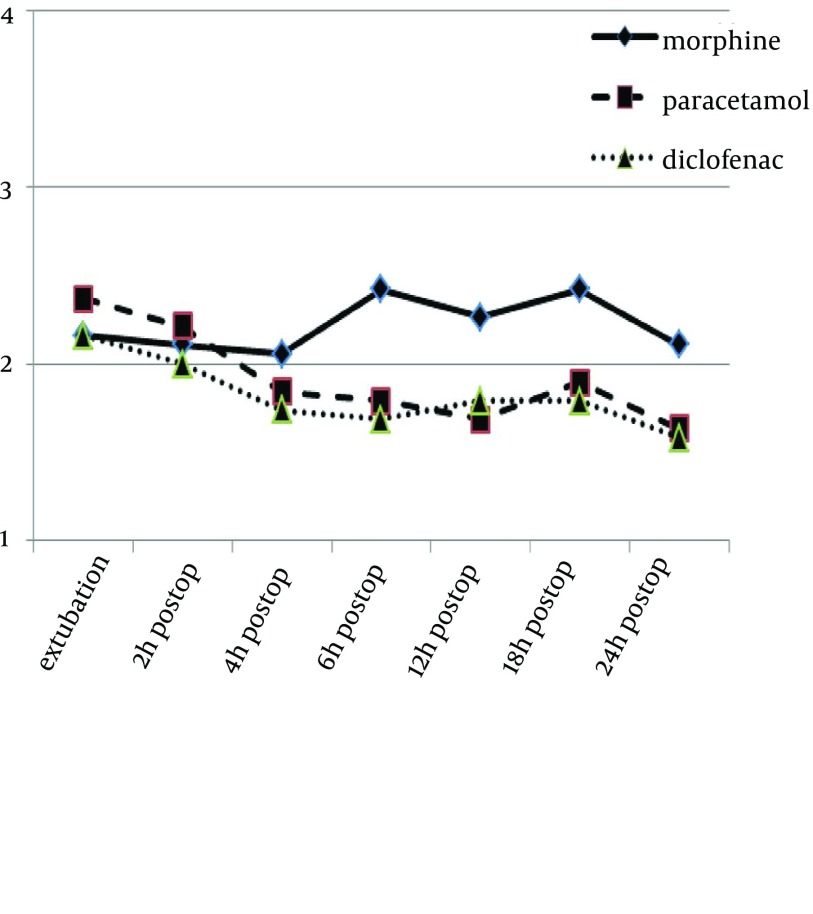
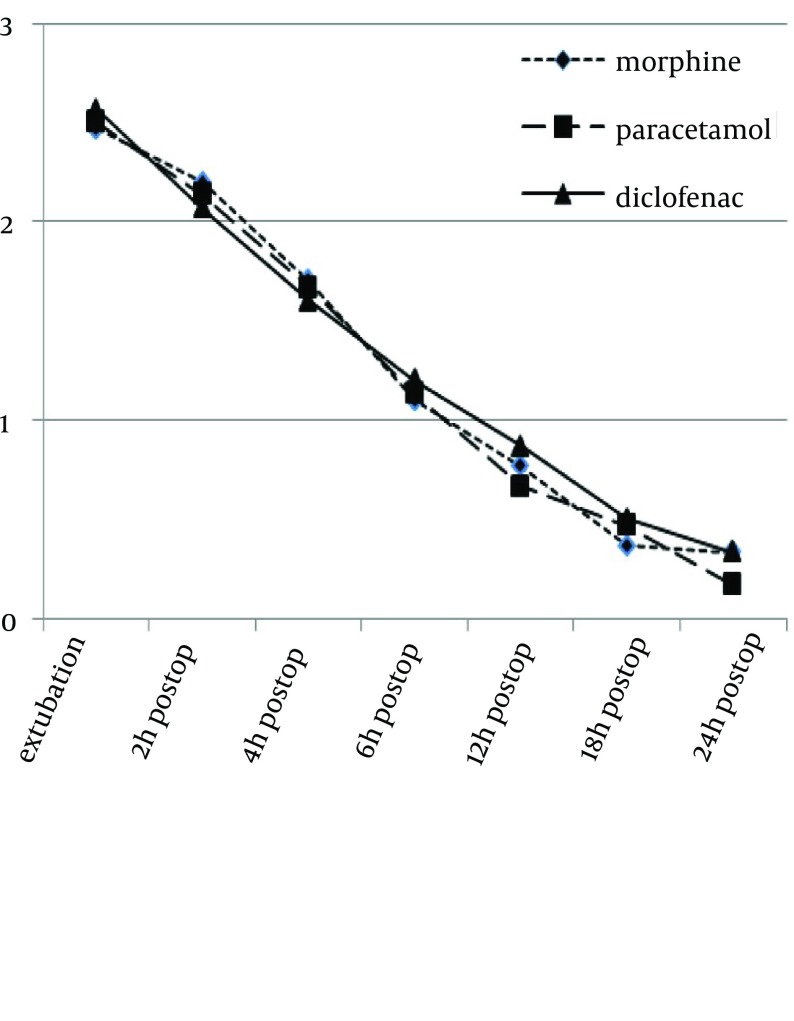
Results: There was no significant difference in pain scores among the three groups (P values, after extubation, at 2, 4, 6, 12, 18 and 24 hours were 0.72, 0.19, 0.21, 0.66, 0.54, 0.56, and 0.25, respectively), although morphine consumption was greater in the morphine group, compared with the other two groups (21.4 ± 7.7 mg in morphine group vs. 14.3 ± 5.8 mg in morphine-paracetamol group and 14.3 ± 3.9 in morphine-diclofenac group; P = 0.001). In morphine group, during the first 24 hours, the patients had lower levels of consciousness (P values, after extubation, at 2, 4, 6, 12, 18 and 24 hour were 0.6, 0.95, 0.28, 0.005, 0.027, 0.022 and 0.004 respectively), even though the incidence of complications was similar among the three groups.
Conclusions: In this study, intravenous paracetamol or diclofenac suppositories, administered for postgastrectomy pain control, decreased morphine consumption by almost 32% and also improved alertness. Nevertheless, the amount of opioids did not affect the incidence of complications.
Keywords: Acetaminophen; Diclofenac; Gastrectomy; Morphine; Pain Management.
Figures
References
-
- Watcha MF, Issioui T, Klein KW, White PF. Costs and effectiveness of rofecoxib, celecoxib, and acetaminophen for preventing pain after ambulatory otolaryngologic surgery. Anesth Analg. 2003;96(4):987–94. - PubMed
-
- Warfield CA, Kahn CH. Acute pain management. Programs in U.S. hospitals and experiences and attitudes among U.S. adults. Anesthesiology. 1995;83(5):1090–4. - PubMed
-
- National Guideline C. Post-operative pain management. Guidelines on pain management. Rockville MD: Agency for Healthcare Research and Quality (AHRQ). 2014.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical