

Quantitative Assessment of the Portal Pressure for the Liver Surgery Using Serological Tests
- PMID: 26587849
- PMCID: PMC4957963
- DOI: 10.1097/SLA.0000000000001460
Quantitative Assessment of the Portal Pressure for the Liver Surgery Using Serological Tests
Abstract
Objective: To establish a reliable equation to predict hepatic venous pressure gradient (HVPG) using serological tests for surgical patients with hepatocellular carcinoma (HCC).
Background: Accurate assessment of portal pressure for surgical patients with HCC is important for safe hepatic resection (HR). The HVPG is regarded as the most reliable method to detect portal hypertension. However, HVPG is not utilized in many medical centers due to invasiveness of procedure.
Methods: Between 2006 and 2008, 171 patients (Correlation cohort), who underwent liver surgery in a tertiary hospital, were enrolled. Preoperative measurements of the HVPG and serological tests were performed simultaneously. Correlation between the HVPG and serological tests were analyzed to establish an equation for calculated HVPG (cHVPG). Between 2008 and 2013, 510 surgical patients (Application cohort) were evaluated, and HR recommended when cHVPG < 10 mm Hg. The outcomes of HR were analyzed to evaluate reliability of the cHVPG for HR.
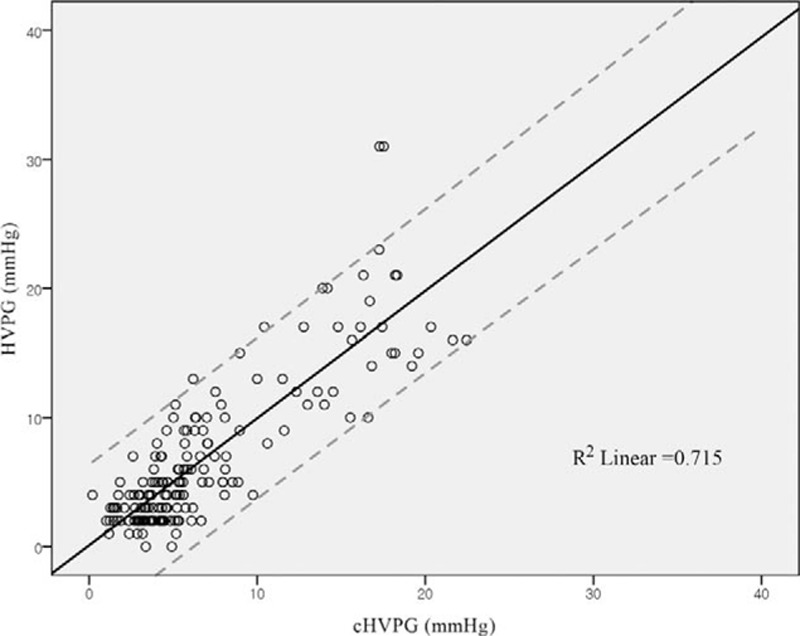
Results: In the correlation cohort, the equation for cHVPG was established using multivariate linear regression analysis; cHVPG (mm Hg) = 0.209 × [ICG-R15 (%)] - 1.646 × [albumin (g/dL)] - 0.01×[platelet count (10)] + 1.669 × [PT-INR] + 8.911. In the application cohort, 425 patients with cHVPG < 10 mm Hg underwent HR. Among them, 357 had favorable value of ICG-R15 < 20% (group A), and 68 had unfavorable value of ICG-R15 ≥ 20% (group B). There was no significant difference in patient demographics, tumor characteristics, operative outcome, and survival rates between group A and B.
Conclusions: The equation for cHVPG of this study was established on statistical reliability. The cHVPG could be useful to predict portal pressure quantitatively for surgical patients with HCC using serological tests.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



References
-
- Groszmann RJ, Garcia-Tsao G, Bosch J, et al. Beta-blockers to prevent gastroesophageal varices in patients with cirrhosis. N Engl J Med 2005; 353:2254–2261. - PubMed
-
- Ripoll C, Groszmann R, Garcia-Tsao G, et al. Hepatic venous pressure gradient predicts clinical decompensation in patients with compensated cirrhosis. Gastroenterology 2007; 133:481–488. - PubMed
-
- Bruix J, Castells A, Bosch J, et al. Surgical resection of hepatocellular carcinoma in cirrhotic patients: prognostic value of preoperative portal pressure. Gastroenterology 1996; 111:1018–1022. - PubMed
-
- Boleslawski E, Petrovai G, Truant S, et al. Hepatic venous pressure gradient in the assessment of portal hypertension before liver resection in patients with cirrhosis. Br J Surg 2012; 99:855–863. - PubMed
-
- Llovet JM, Burroughs A, Bruix J. Hepatocellular carcinoma. Lancet 2003; 362:1907–1917. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
