

Residual Cardiovascular Risk in Individuals on Blood Pressure-Lowering Treatment
- PMID: 26588944
- PMCID: PMC4845218
- DOI: 10.1161/JAHA.115.002155
Residual Cardiovascular Risk in Individuals on Blood Pressure-Lowering Treatment
Abstract
Background: Hypertensive individuals on blood pressure (BP)-lowering treatment with BP in the normal or high-normal range have higher cardiovascular risk than untreated persons with usual BP in the same range. This residual risk (relative and absolute) is not well quantified and may be attributable in part to the higher burden of subclinical disease in treated individuals.
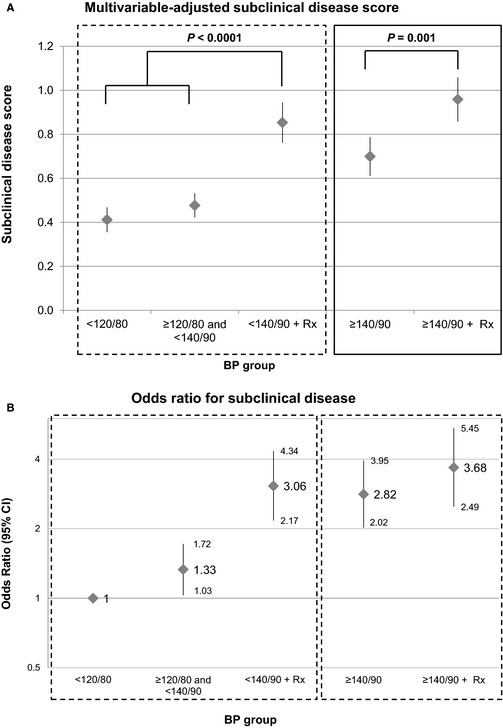
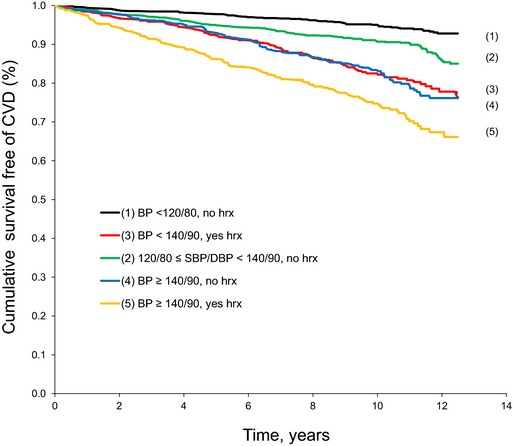
Methods and results: We assigned 3024 Framingham Offspring Cohort participants to 5 categories based on systolic BP (SBP) and diastolic BP (DBP) and use of BP-lowering treatment: (1) untreated SBP/DBP <120/80 mm Hg; (2) untreated SBP/DB ≥120/80 to <140/90 mm Hg; (3) treated SBP/DBP <140/90 mm Hg; (4) untreated SBP/DBP ≥140/90 mm Hg; and (5) treated SBP/DBP ≥140/90 mm Hg. A composite subclinical disease score was constructed, including information on left ventricular hypertrophy, systolic dysfunction, carotid ultrasound abnormality, peripheral artery disease, and microalbuminuria. The prevalence of subclinical disease rose across BP groups, as did the event rates for incident cardiovascular disease (449 events, median follow-up of 11 years; group 1, 0.65 event per 100 person-years; group 5, 3.20 events per 100 person-years; P<0.0001 for trend). On multivariable adjustment, treated hypertensives in groups 3 and 5 had 50% (95% CI 13% to 99%) and 28% (95% CI -6% to 73%) higher hazards, respectively, of developing cardiovascular disease compared with their untreated counterparts with similar levels of BP (groups 1 and 2 and group 4, respectively). The increased risk of cardiovascular disease in treated hypertensives was attributable in part to greater subclinical disease burden.
Conclusions: Treated hypertensives have higher subclinical cardiovascular disease burden, which partly explains their higher cardiovascular disease risk compared with untreated persons with similar BP levels.
Keywords: blood pressure; cardiovascular disease; subclinical disease.
© 2015 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Vasan RS, Larson MG, Leip EP, Evans JC, O'Donnell CJ, Kannel WB, Levy D. Impact of high‐normal blood pressure on the risk of cardiovascular disease. N Engl J Med. 2001;345:1291–1297. - PubMed
-
- Stamler J, Stamler R, Neaton JD. Blood pressure, systolic and diastolic, and cardiovascular risks. US population data. Arch Intern Med. 1993;153:598–615. - PubMed
-
- Staessen JA, Gasowski J, Wang JG, Thijs L, Den Hond E, Boissel JP, Coope J, Ekbom T, Gueyffier F, Liu L, Kerlikowske K, Pocock S, Fagard RH. Risks of untreated and treated isolated systolic hypertension in the elderly: meta‐analysis of outcome trials. Lancet. 2000;355:865–872. - PubMed
-
- Collins R, Peto R, MacMahon S, Hebert P, Fiebach NH, Eberlein KA, Godwin J, Qizilbash N, Taylor JO, Hennekens CH. Blood pressure, stroke, and coronary heart disease. Part 2, short‐term reductions in blood pressure: overview of randomised drug trials in their epidemiological context. Lancet. 1990;335:827–838. - PubMed
-
- Stumpe KO, Agabiti‐Rosei E, Zielinski T, Schremmer D, Scholze J, Laeis P, Schwandt P, Ludwig M. Carotid intima‐media thickness and plaque volume changes following 2‐year angiotensin II‐receptor blockade. The multicentre olmesartan atherosclerosis regression evaluation (MORE) study. Ther Adv Cardiovasc Dis. 2007;1:97–106. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
