

CoCStom trial: study protocol for a randomised trial comparing completeness of adjuvant chemotherapy after early versus late diverting stoma closure in low anterior resection for rectal cancer
- PMID: 26589718
- PMCID: PMC4654836
- DOI: 10.1186/s12885-015-1838-0
CoCStom trial: study protocol for a randomised trial comparing completeness of adjuvant chemotherapy after early versus late diverting stoma closure in low anterior resection for rectal cancer
Abstract
Background: Current evidence supports a diverting stoma in patients undergoing low anterior resection with total mesorectal excision for rectal cancer as it reduces clinical severity of anastomotic leakage. However, relevant stoma morbidity after rectal cancer surgery exists and has a significant impact on quality of life. Moreover, a diverting stoma has an influence on completeness of chemotherapy but it remains unclear in which way. There is no evidence regarding optimal timing for stoma closure in relation to adjuvant chemotherapy. Two randomised controlled trials have studied early stoma closure after low anterior resection in patients with rectal cancer, one of them showing that early closure around day 8 after resection is possible without increasing morbidity.
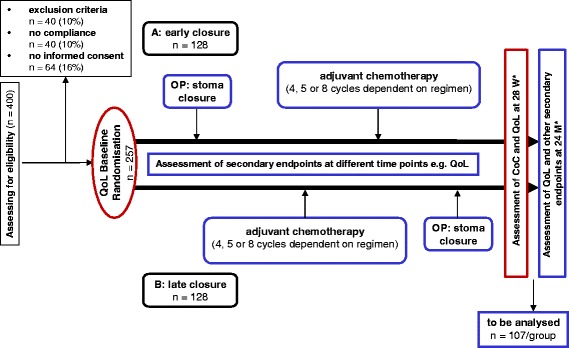
Methods/design: CoCStom is a randomised multicentre trial comparing completeness of adjuvant chemotherapy as primary endpoint after early (8-10 days after resection, before starting adjuvant therapy) versus late (~26 weeks after resection and completion of adjuvant therapy) stoma closure in patients with locally advanced rectal cancer undergoing low anterior resection after neoadjuvant therapy. After exclusion of post-operative anastomotic leakage 257 patients from 30 German hospitals are planned to be included in order to assure a power of 80% for the confirmatory analysis of at least 214 evaluable cases. An absolute increase of 20% for the rate of completely administered adjuvant chemotherapy is regarded as a clinically meaningful step forward and serves as basis for sample size calculation. Quality of life, stoma-related complications, individual completeness of chemotherapy rate, percentage of patients stopping adjuvant therapy or undergoing dose modifications or delay, oncological outcomes, cumulative days of hospitalisation and number of readmissions, rate of symptomatic anastomotic leaks after stoma closure, mortality, post-operative complications and toxicity of adjuvant chemotherapy are secondary endpoints.
Discussion: The CoCStom trial aims to clarify optimal timing of stoma closure in the context of adjuvant chemotherapy. Depending on the results of the trial, patients could benefit either from early or late stoma closure in regard to long term oncological survival due to a higher rate of completeness of adjuvant chemotherapy treatment and thus better effectiveness.
Trial registration: German Clinical Trials Register, DRKS00005113. Registered 28 August 2013.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
