

Food Access, Chronic Kidney Disease, and Hypertension in the U.S
- PMID: 26590940
- PMCID: PMC4656149
- DOI: 10.1016/j.amepre.2015.07.017
Food Access, Chronic Kidney Disease, and Hypertension in the U.S
Abstract
Introduction: Greater distance to full-service supermarkets and low income may impair access to healthy diets and contribute to chronic kidney disease (CKD) and hypertension. The study aim was to determine relationships among residence in a "food desert," low income, CKD, and blood pressure.
Methods: Adults in the 2003-2010 National Health and Nutrition Examination Survey (N=22,173) were linked to food desert data (www.ers.usda.gov) by Census Tracts. Food deserts have low median income and are further from a supermarket or large grocery store (>1 mile in urban areas, >10 miles in rural areas). Weighted regression was used to determine the association of residence in a food desert and family income with dietary intake; systolic blood pressure (SBP); and odds of CKD. Data analysis was performed in 2014-2015.
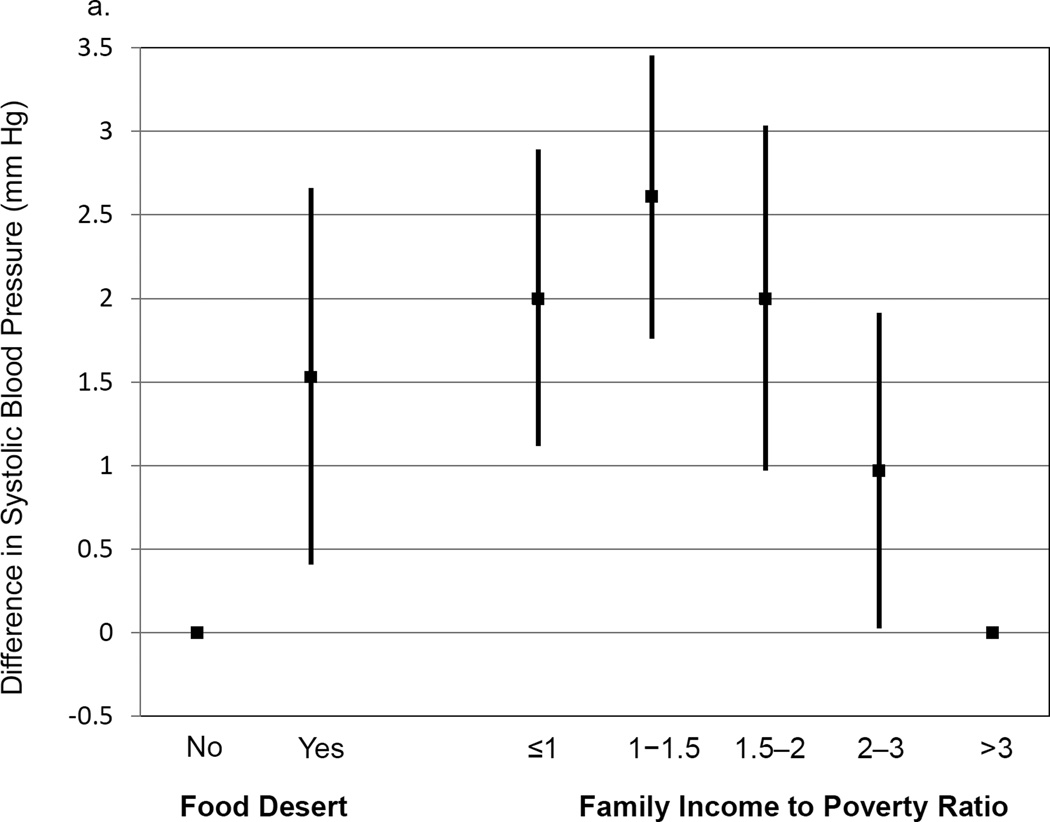
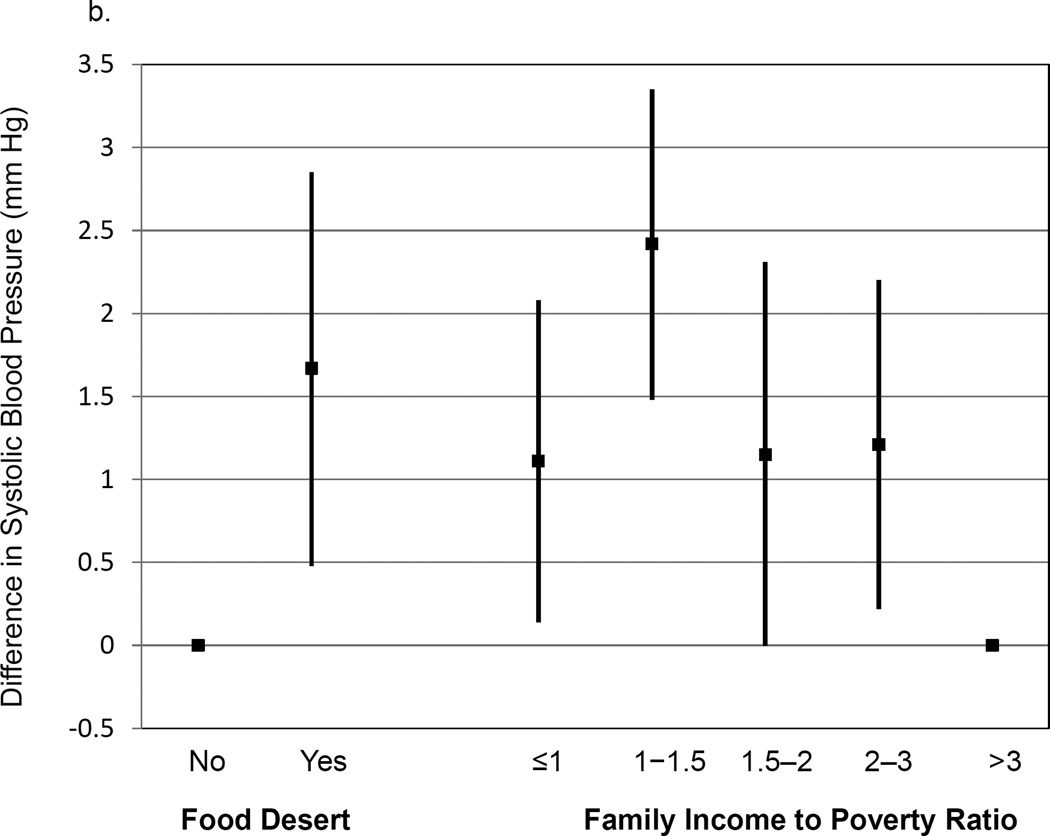
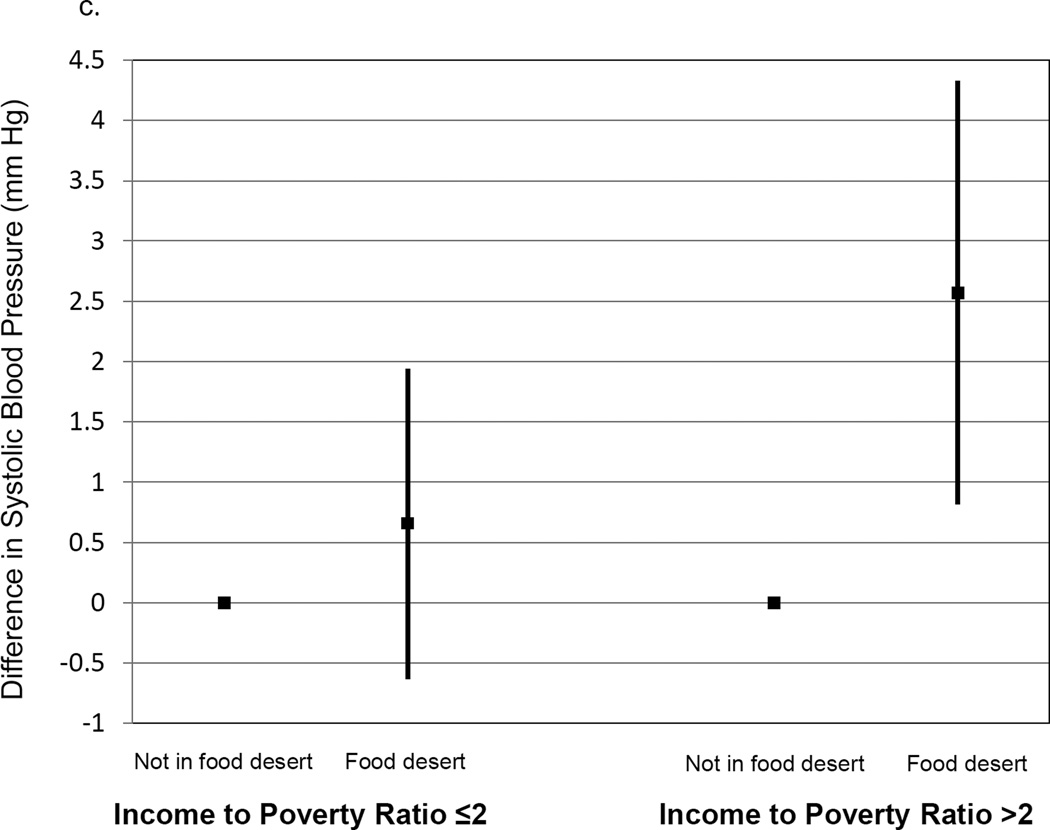
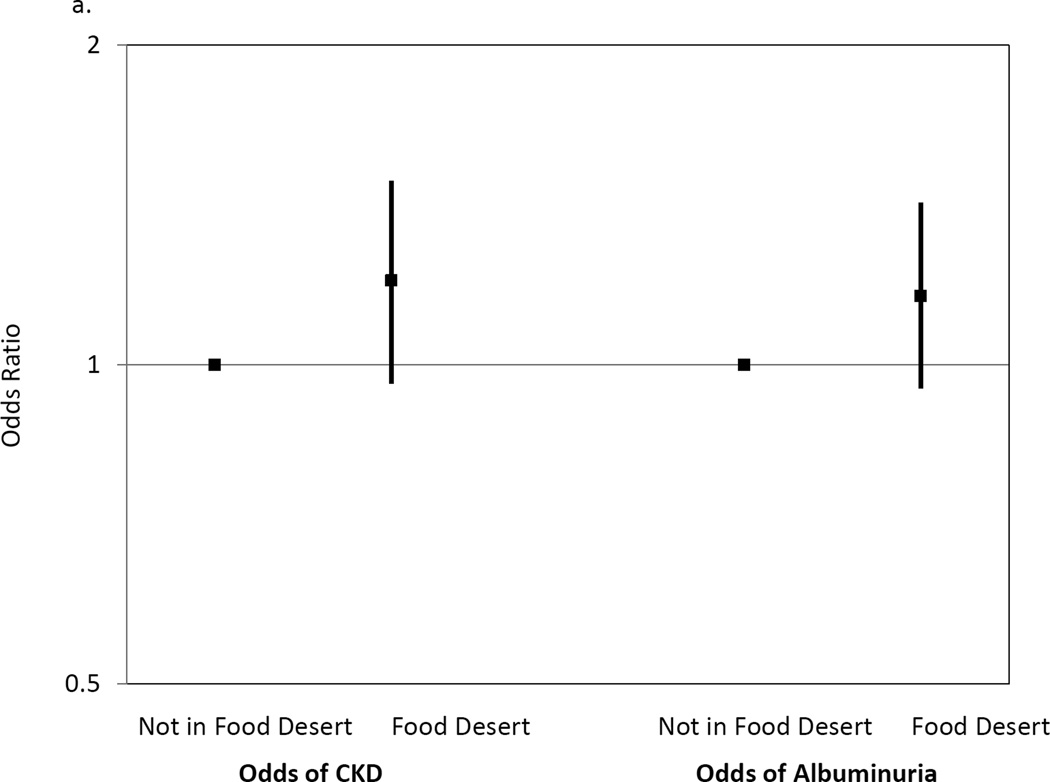
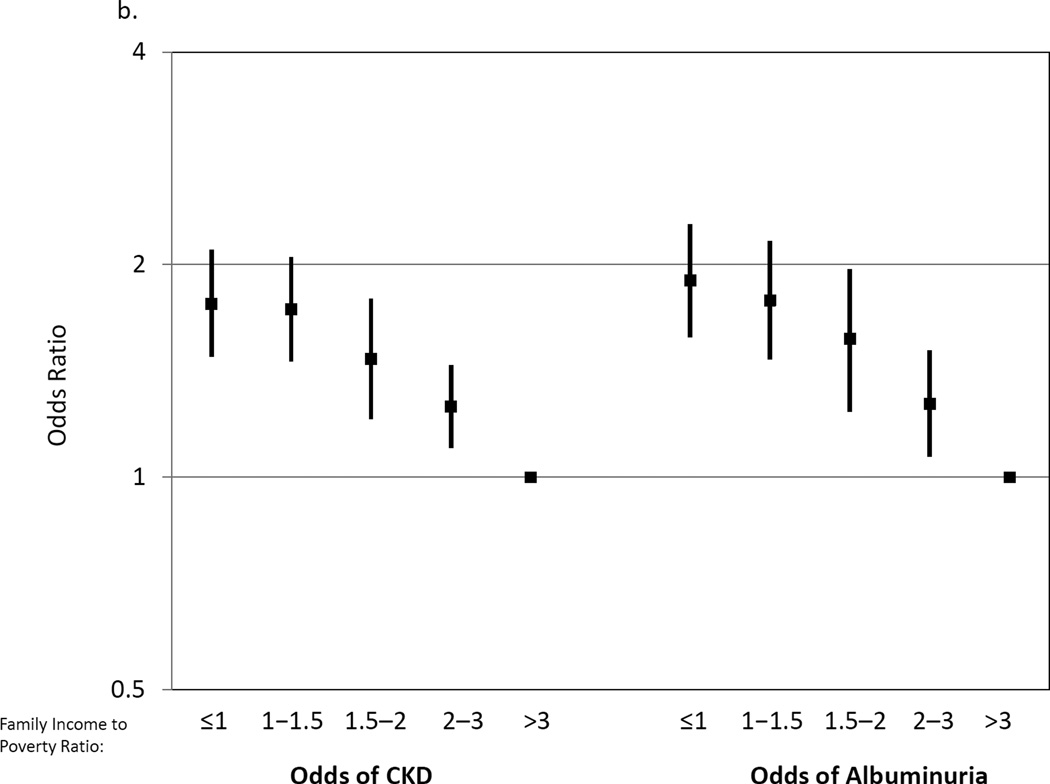
Results: Compared with those not in food deserts, participants residing in food deserts had lower levels of serum carotenoids (p<0.01), a biomarker of fruit and vegetable intake, and higher SBP (1.53 mmHg higher, 95% CI=0.41, 2.66) after adjustment for demographics and income. Residence in a food desert was not associated with odds of CKD (OR=1.20, 95% CI=0.96, 1.49). Lower, versus higher, income was associated with lower serum carotenoids (p<0.01) and higher SBP (2.00 mmHg higher for income-poverty ratio ≤1 vs >3, 95% CI=1.12, 2.89), but also greater odds of CKD (OR=1.76 for income-poverty ratio ≤1 vs >3, 95% CI=1.48, 2.10).
Conclusions: Limited access to healthy food due to geographic or financial barriers could be targeted for prevention of CKD and hypertension.
Copyright © 2015 American Journal of Preventive Medicine. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Supermarket Proximity and Risk of Hypertension, Diabetes, and CKD: A Retrospective Cohort Study.Am J Kidney Dis. 2023 Feb;81(2):168-178. doi: 10.1053/j.ajkd.2022.07.008. Epub 2022 Sep 2. Am J Kidney Dis. 2023. PMID: 36058428 Free PMC article.
-
Food Insecurity, CKD, and Subsequent ESRD in US Adults.Am J Kidney Dis. 2017 Jul;70(1):38-47. doi: 10.1053/j.ajkd.2016.10.035. Epub 2017 Feb 16. Am J Kidney Dis. 2017. PMID: 28215947 Free PMC article.
-
Effect of food insecurity on chronic kidney disease in lower-income Americans.Am J Nephrol. 2014;39(1):27-35. doi: 10.1159/000357595. Epub 2014 Jan 8. Am J Nephrol. 2014. PMID: 24434743 Free PMC article.
-
Contextual poverty, nutrition, and chronic kidney disease.Adv Chronic Kidney Dis. 2015 Jan;22(1):31-8. doi: 10.1053/j.ackd.2014.05.005. Adv Chronic Kidney Dis. 2015. PMID: 25573510 Free PMC article. Review.
-
Social Determinants of CKD Hotspots.Semin Nephrol. 2019 May;39(3):256-262. doi: 10.1016/j.semnephrol.2019.02.003. Semin Nephrol. 2019. PMID: 31054624 Free PMC article. Review.
Cited by
-
Disparities in access to food and chronic obstructive pulmonary disease (COPD)-related outcomes: a cross-sectional analysis.BMC Pulm Med. 2021 Apr 27;21(1):139. doi: 10.1186/s12890-021-01485-8. BMC Pulm Med. 2021. PMID: 33906617 Free PMC article.
-
Washington State's Fruit and Vegetable Prescription Program: Improving Affordability of Healthy Foods for Low-Income Patients.Prev Chronic Dis. 2019 Jul 18;16:E91. doi: 10.5888/pcd16.180617. Prev Chronic Dis. 2019. PMID: 31322108 Free PMC article.
-
World Heart Federation Roadmap for Hypertension - A 2021 Update.Glob Heart. 2021 Sep 10;16(1):63. doi: 10.5334/gh.1066. eCollection 2021. Glob Heart. 2021. PMID: 34692387 Free PMC article. Review.
-
Burden, access, and disparities in kidney disease.Pediatr Nephrol. 2019 Apr;34(4):541-548. doi: 10.1007/s00467-019-4197-2. Pediatr Nephrol. 2019. PMID: 30758679
-
Disparities in neighborhood food environment and cognitive decline among US older adults: a cohort study.BMC Med. 2025 May 6;23(1):259. doi: 10.1186/s12916-025-04091-1. BMC Med. 2025. PMID: 40325457 Free PMC article.
References
-
- Coresh J, Selvin E, Stevens LA, et al. Prevalence of Chronic Kidney Disease in the United States. JAMA. 2007;298(17):2038–2047. http://dx.doi.org/10.1001/jama.298.17.2038. - DOI - PubMed
-
- U.S. Burden of Disease Collaborators. The State of U.S. Health, 1990–2010, Burden of Diseases, Injuries and Risk Factors. JAMA. 2013;310(6):591–606. http://dx.doi.org/10.1001/jama.2013.13805. - DOI - PMC - PubMed
-
- Crews D, Plantinga L, Miller ER, 3rd, et al. Prevalence of chronic kidney disease in persons with undiagnosed or prehypertension in the United States. Hypertension. 2010;55:1102–1109. http://dx.doi.org/10.1161/HYPERTENSIONAHA.110.150722. - DOI - PMC - PubMed
-
- Saran R, Hedgeman E, Plantinga L, et al. Establishing a national chronic kidney disease surveillance system for the United States. Clin J Am Soc Nephrol. 2010;5(1):152–161. http://dx.doi.org/10.2215/CJN.05480809. - DOI - PubMed
-
- Mensah GA, Mokdad AH, Ford ES, Greenlund KJ, Croft JB. State of Disparities in Cardiovascular Health in the United States. Circulation. 2005;111(10):1233–1241. http://dx.doi.org/10.1161/01.CIR.0000158136.76824.04. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
