

Evaluation of an mHealth Medication Regimen Self-Management Program for African American and Hispanic Uncontrolled Hypertensives
- PMID: 26593951
- PMCID: PMC4695862
- DOI: 10.3390/jpm5040389
Evaluation of an mHealth Medication Regimen Self-Management Program for African American and Hispanic Uncontrolled Hypertensives
Abstract
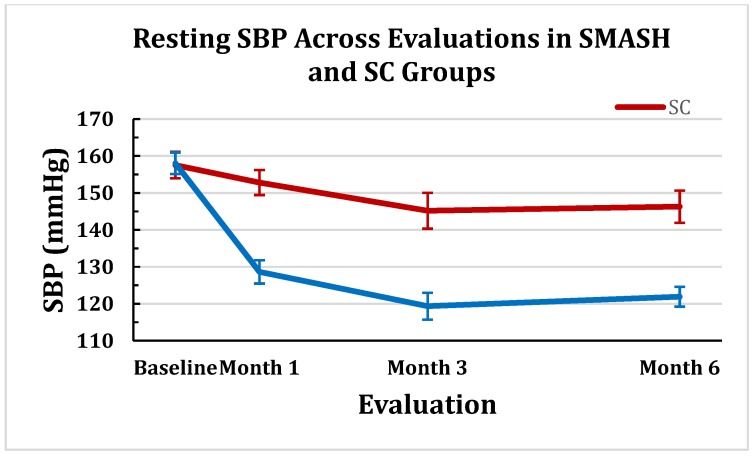
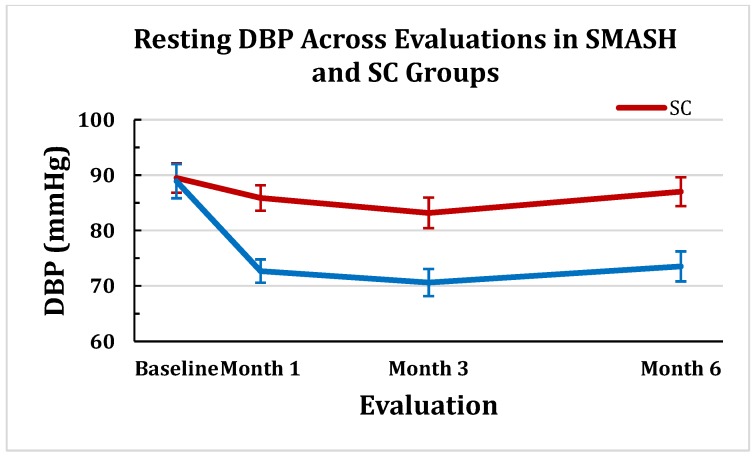
African Americans and Hispanics have disproportionate rates of uncontrolled essential hypertension (EH) compared to Non-Hispanic Whites. Medication non-adherence (MNA) is the leading modifiable behavior to improved blood pressure (BP) control. The Smartphone Medication Adherence Stops Hypertension (SMASH) program was developed using a patient-centered, theory-guided, iterative design process. Electronic medication trays provided reminder signals, and Short Message Service [SMS] messaging reminded subjects to monitor BP with Bluetooth-enabled monitors. Motivational and reinforcement text messages were sent to participants based upon levels of adherence. Thirty-eight African-American (18) and Hispanic (20) uncontrolled hypertensives completed clinic-based anthropometric and resting BP evaluations prior to randomization, and again at months 1, 3 and 6. Generalized linear mixed modeling (GLMM) revealed statistically significant time-by-treatment interactions (p < 0.0001) indicating significant reductions in resting systolic blood pressure (SBP) and diastolic blood pressure (DBP) for the SMASH group vs. the standard care (SC) control group across all time points. 70.6% of SMASH subjects vs. 15.8% of the SC group reached BP control (< 140/90 mmH) at month 1 (p < 0.001). At month 6, 94.4% of the SMASH vs. 41.2% of the SC group exhibited controlled BP (p < 0.003). Our findings provide encouraging evidence that efficacious mHealth, chronic disease, medical regimen, self-management programs can be developed following principles of patient-centered, theory-guided design.
Keywords: essential hypertension; iterative design; mHealth; patient centered.
Figures
References
-
- James P.A., Oparil S., Carter B.L., Cushman W.C., Dennison-Himmelfarb C., Handler J., Lackland D.T., LeFevre M.L., MacKenzie T.D., Ogedegbe O., et al. 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the eighth joint national committee (jnc 8) JAMA. 2014;311:507–520. doi: 10.1001/jama.2013.284427. - DOI - PubMed
-
- Yoon S.S., Ostchega Y., Louis T. Recent trends in the prevalence of high blood pressure and its treatment and control, 1999–2008. NCHS Data Brief. 2010;48:1–8. - PubMed
-
- Keenan N.L., Rosendorf K.A., Centers for Disease Control and Prevention (CDC) Prevalence of hypertension and controlled hypertension—united states, 2005–2008. MMWR Surveill. Summ. 2011;60:94–97. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
