

Bilateral Continuous Automated Distraction Osteogenesis: Proof of Principle
- PMID: 26594967
- PMCID: PMC4662050
- DOI: 10.1097/SCS.0000000000001996
Bilateral Continuous Automated Distraction Osteogenesis: Proof of Principle
Abstract
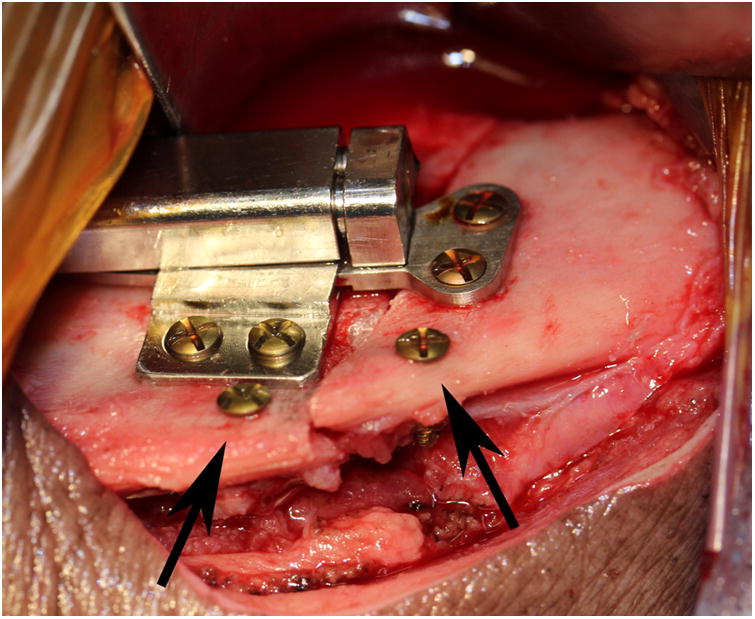
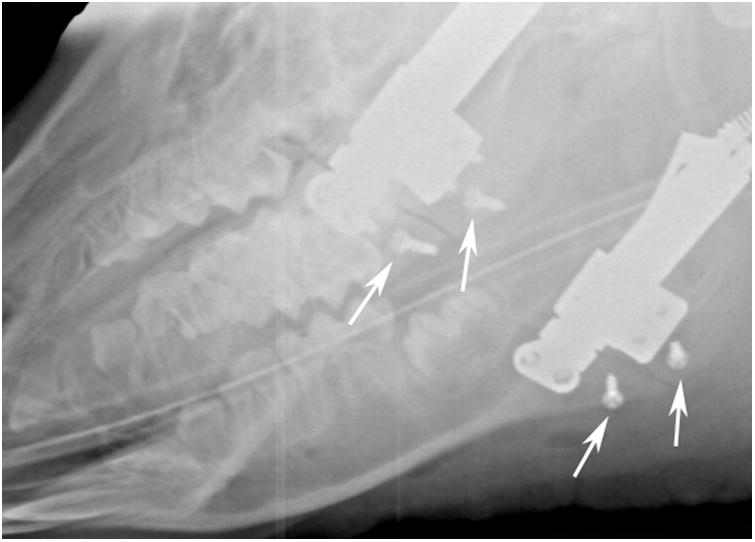
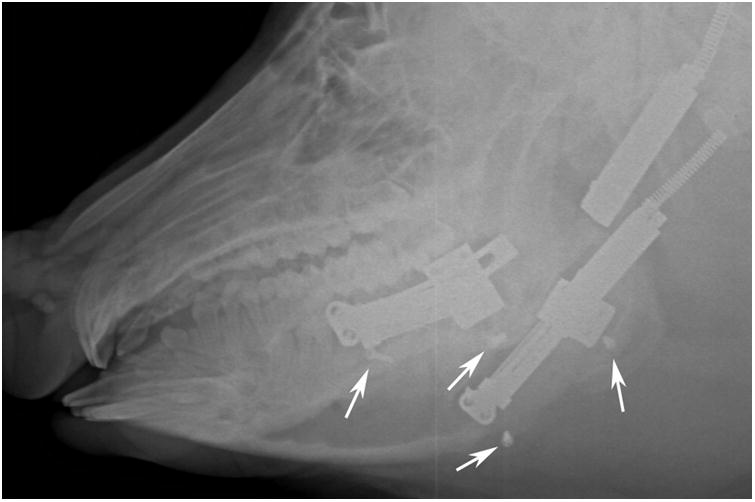
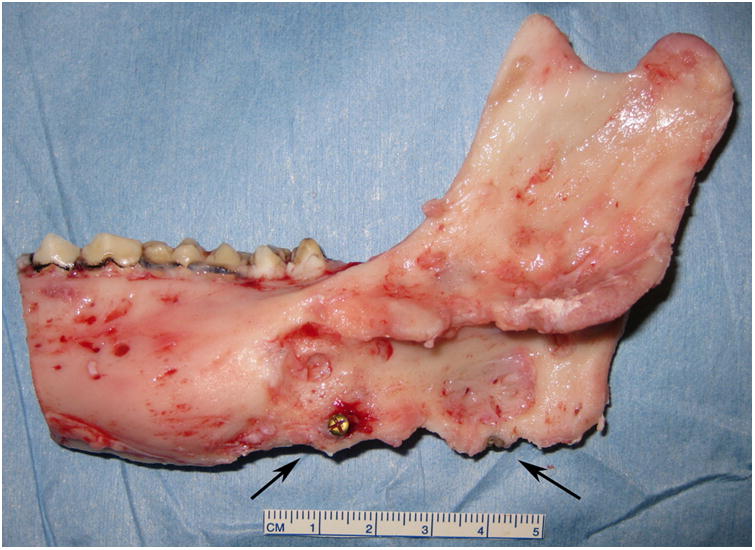
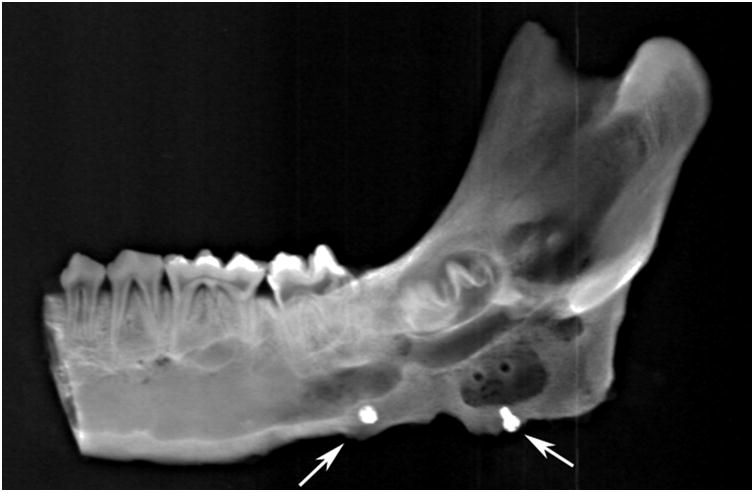
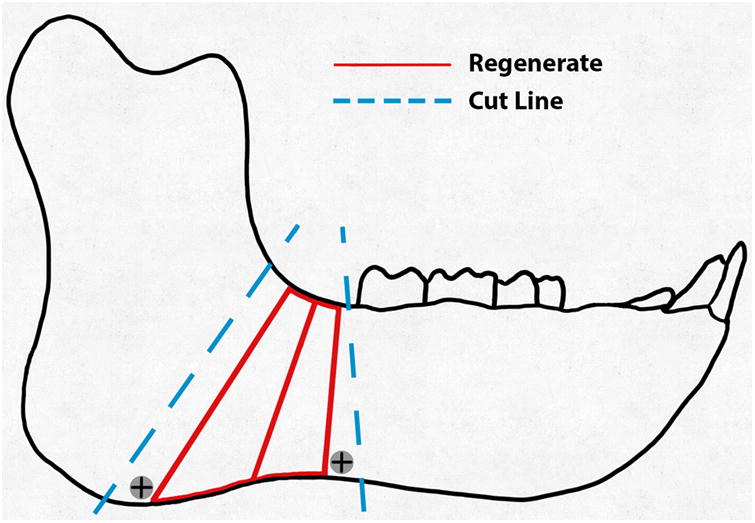
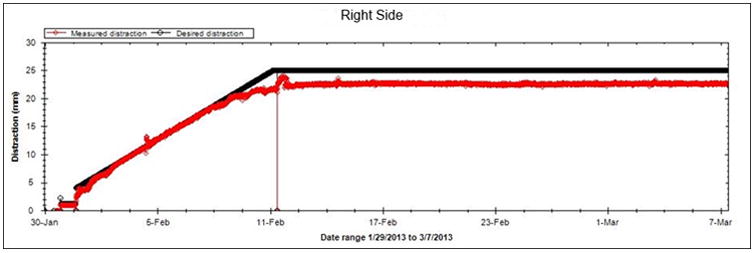
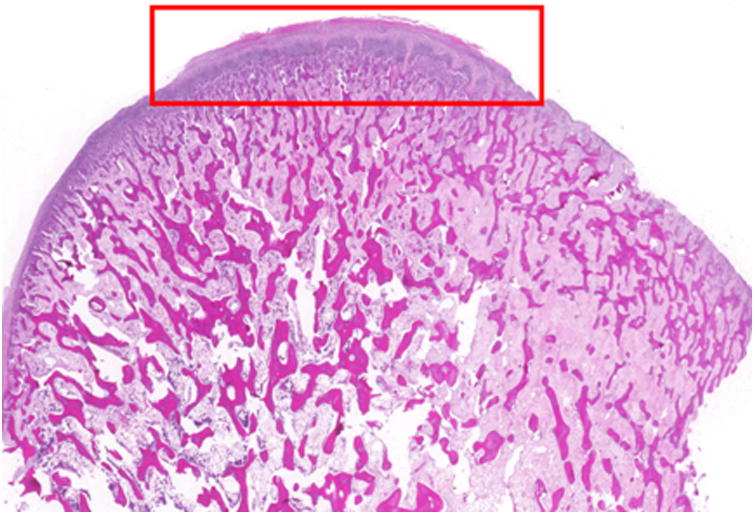
The purpose of this study was to demonstrate that automated, continuous, curvilinear distraction osteogenesis (DO) in a minipig model is effective when performed bilaterally, at rates up to 3 mm/day, to achieve clinically relevant lengthening. A Yucatan minipig in the mixed dentition phase underwent bilaterally, at a continuous DO at a rate of 2 mm/day at the center of rotation; 1.0 and 3.0 mm/day at the superior and inferior regions, respectively. The distraction period was 13 days with no latency period. Vector and rate of distraction were remotely monitored without radiographs, using the device sensor. After fixation and euthanasia, the mandible and digastric muscles were harvested. The ex vivo appearance, stability, and radiodensity of the regenerate were evaluated using a semiquantitative scale. Percent surface area (PSA) occupied by bone, fibrous tissue, cartilage, and hematoma were calculated using histomorphometrics. The effects of DO on the digastric muscles and mandibular condyles were assessed via microscopy, and degenerative changes were quantified. The animal was distracted to 21 mm and 24 mm on the right and left sides, respectively. Clinical appearance, stability, and radiodensity were scored as "3" bilaterally indicating osseous union. The total PSA occupied by bone (right = 75.53 ± 2.19%; left PSA = 73.11 ± 2.18%) approached that of an unoperated mandible (84.67 ± 0.86%). Digastric muscles and condyles showed negligible degenerative or abnormal histologic changes. This proof of principle study is the first report of osseous healing with no ill-effect on associated soft tissue and the mandibular condyle using bilateral, automated, continuous, and curvilinear DO at rates up to 3 mm/day. The model approximates potential human application of continuous automated distraction with a semiburied device.
Figures


References
-
- Ilizarov GA. The principles of the Ilizarov method. Bull Hosp Jt Dis Orthop Inst. 1988;48:1–11. - PubMed
-
- Ilizarov GA. The tension-stress effect on the genesis and growth of tissues: Part II The influence of the rate and frequency of distraction. Clin Orthop Relat Res. 1989;239:263–285. - PubMed
-
- Ilizarov GA. The tension-stress effect on the genesis and growth of tissues. Part I.The influence of stability of fixation and soft-tissue preservation. Clin Orthop Relat Res. 1989;238:249–281. - PubMed
-
- Ilizarov GA. Clinical application of the tension-stress effect for limb lengthening. Clin Orthop Relat Res. 1990;250:8–26. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
