

In Vivo Microdialysis To Determine Subcutaneous Interstitial Fluid Penetration and Pharmacokinetics of Fluconazole in Intensive Care Unit Patients with Sepsis
- PMID: 26596947
- PMCID: PMC4750683
- DOI: 10.1128/AAC.02461-15
In Vivo Microdialysis To Determine Subcutaneous Interstitial Fluid Penetration and Pharmacokinetics of Fluconazole in Intensive Care Unit Patients with Sepsis
Abstract
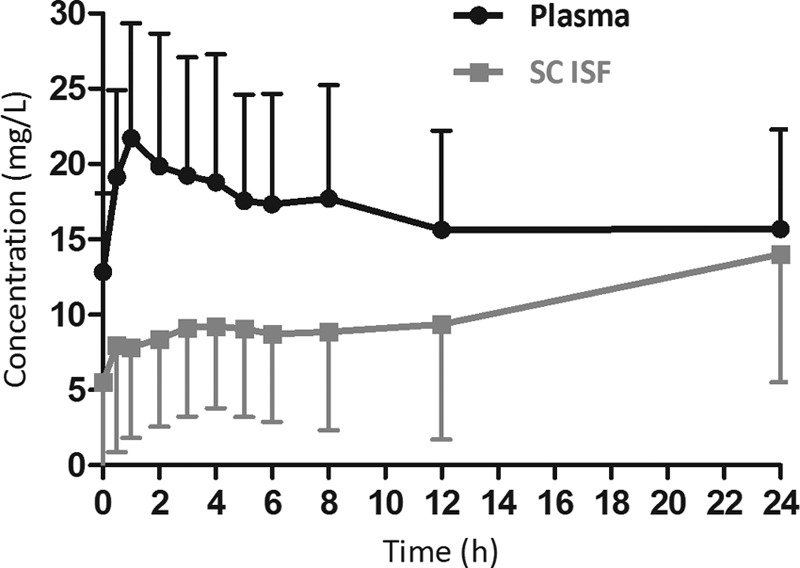
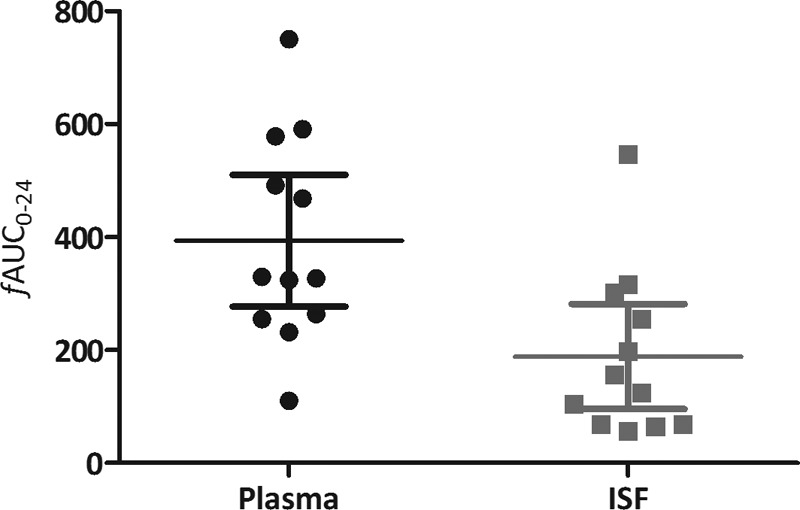
The objective of the study was to describe the subcutaneous interstitial fluid (ISF) pharmacokinetics of fluconazole in critically ill patients with sepsis. This prospective observational study was conducted at two tertiary intensive care units in Australia. Serial fluconazole concentrations were measured over 24 h in plasma and subcutaneous ISF using microdialysis. The concentrations in plasma and microdialysate were measured using a validated high-performance liquid chromatography system with electrospray mass spectrometer detector method. Noncompartmental pharmacokinetic analysis was performed. Twelve critically ill patients with sepsis were enrolled. The mean in vivo fluconazole recovery rates ± standard deviation (SD) for microdialysis were 51.4% ± 16.1% with a mean (±SD) fluconazole ISF penetration ratio of 0.52 ± 0.30 (coefficient of variation, 58%). The median free plasma area under the concentration-time curve from 0 to 24 h (AUC0-24) was significantly higher than the median ISF AUC0-24 (340.4 versus 141.1 mg · h/liter; P = 0.004). There was no statistical difference in median fluconazole ISF penetration between patients receiving and not receiving vasopressors (median, 0.28 versus 0.78; P = 0.106). Both minimum and the maximum concentrations of drug in serum (Cmax and Cmin) showed a significant correlation with the fluconazole plasma exposure (Cmax, R(2) = 0.86, P < 0.0001; Cmin, R(2) = 0.75, P < 0.001). Our data suggest that fluconazole was distributed variably, but incompletely, from plasma into subcutaneous interstitial fluid in this cohort of critically ill patients with sepsis. Given the variability of fluconazole interstitial fluid exposures and lack of clinically identifiable factors by which to recognize patients with reduced distribution/exposure, we suggest higher than standard doses to ensure that drug exposure is adequate at the site of infection.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures

Similar articles
-
Influence of sustained low-efficiency diafiltration (SLED-f) on interstitial fluid concentrations of fluconazole in a critically ill patient: Use of microdialysis.Int J Antimicrob Agents. 2015 Jul;46(1):121-4. doi: 10.1016/j.ijantimicag.2015.02.017. Epub 2015 Mar 28. Int J Antimicrob Agents. 2015. PMID: 25888463
-
Effect of Obesity on the Population Pharmacokinetics of Fluconazole in Critically Ill Patients.Antimicrob Agents Chemother. 2016 Oct 21;60(11):6550-6557. doi: 10.1128/AAC.01088-16. Print 2016 Nov. Antimicrob Agents Chemother. 2016. PMID: 27550344 Free PMC article.
-
Human subcutaneous tissue distribution of fluconazole: comparison of microdialysis and suction blister techniques.Br J Clin Pharmacol. 2003 Nov;56(5):551-61. doi: 10.1046/j.1365-2125.2003.01930.x. Br J Clin Pharmacol. 2003. PMID: 14651730 Free PMC article.
-
Pharmacokinetic evaluation of fluconazole in critically ill patients.Expert Opin Drug Metab Toxicol. 2011 Nov;7(11):1431-40. doi: 10.1517/17425255.2011.615309. Epub 2011 Sep 2. Expert Opin Drug Metab Toxicol. 2011. PMID: 21883033 Review.
-
Candida and candidaemia. Susceptibility and epidemiology.Dan Med J. 2013 Nov;60(11):B4698. Dan Med J. 2013. PMID: 24192246 Review.
Cited by
-
Pharmacokinetic and pharmacodynamic considerations for antifungal therapy optimisation in the treatment of intra-abdominal candidiasis.Crit Care. 2023 Nov 20;27(1):449. doi: 10.1186/s13054-023-04742-w. Crit Care. 2023. PMID: 37981676 Free PMC article. Review.
-
Utility of Microdialysis in Infectious Disease Drug Development and Dose Optimization.AAPS J. 2017 Mar;19(2):334-342. doi: 10.1208/s12248-016-0020-1. Epub 2016 Dec 9. AAPS J. 2017. PMID: 27943149 Review.
-
Challenges in Antifungal Therapy in Diabetes Mellitus.J Clin Med. 2020 Sep 6;9(9):2878. doi: 10.3390/jcm9092878. J Clin Med. 2020. PMID: 32899911 Free PMC article.
-
Choosing the Right Antifungal Agent in ICU Patients.Adv Ther. 2019 Dec;36(12):3308-3320. doi: 10.1007/s12325-019-01115-0. Epub 2019 Oct 15. Adv Ther. 2019. PMID: 31617055 Free PMC article.
-
Diagnosis and management of invasive candidiasis in the ICU: an updated approach to an old enemy.Crit Care. 2016 May 27;20(1):125. doi: 10.1186/s13054-016-1313-6. Crit Care. 2016. PMID: 27230564 Free PMC article. Review.
References
-
- Wisplinghoff H, Ebbers J, Geurtz L, Stefanik D, Major Y, Edmond MB, Wenzel RP, Seifert H. 2014. Nosocomial bloodstream infections due to Candida spp. in the USA: species distribution, clinical features and antifungal susceptibilities. Int J Antimicrob Agents 43:78–81. doi:10.1016/j.ijantimicag.2013.09.005. - DOI - PubMed
-
- Guery BP, Arendrup MC, Auzinger G, Azoulay E, Borges Sa M, Johnson EM, Muller E, Putensen C, Rotstein C, Sganga G, Venditti M, Zaragoza Crespo R, Kullberg BJ. 2009. Management of invasive candidiasis and candidemia in adult non-neutropenic intensive care unit patients. Part I. Epidemiology and diagnosis. Intensive Care Med 35:55–62. doi:10.1007/s00134-008-1338-7. - DOI - PubMed
-
- Vincent JL, Rello J, Marshall J, Silva E, Anzueto A, Martin CD, Moreno R, Lipman J, Gomersall C, Sakr Y, Reinhart K, EPIC II Group of Investigators . 2009. International study of the prevalence and outcomes of infection in intensive care units. JAMA 302:2323–2329. doi:10.1001/jama.2009.1754. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
