

Relation of Central Arterial Stiffness to Incident Heart Failure in the Community
- PMID: 26597152
- PMCID: PMC4845230
- DOI: 10.1161/JAHA.115.002189
Relation of Central Arterial Stiffness to Incident Heart Failure in the Community
Abstract
Background: Arterial stiffness, pressure pulsatility, and wave reflection are associated with cardiovascular disease. Left ventricular function is coupled to proximal aortic properties, but the association of central aortic stiffness and hemodynamics with incident clinical heart failure (HF) is not well described.
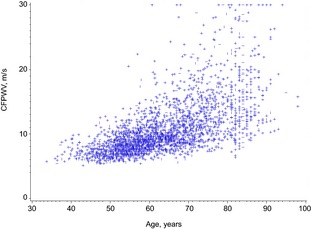
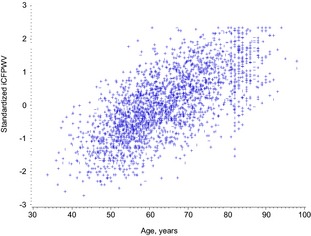
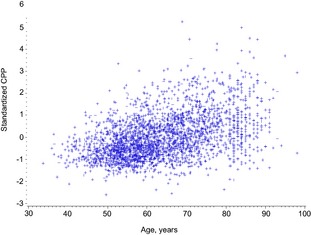
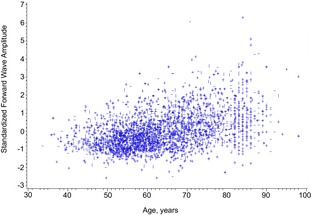
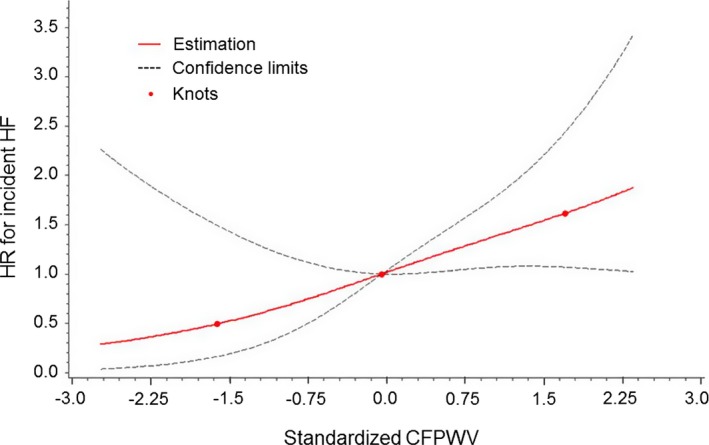
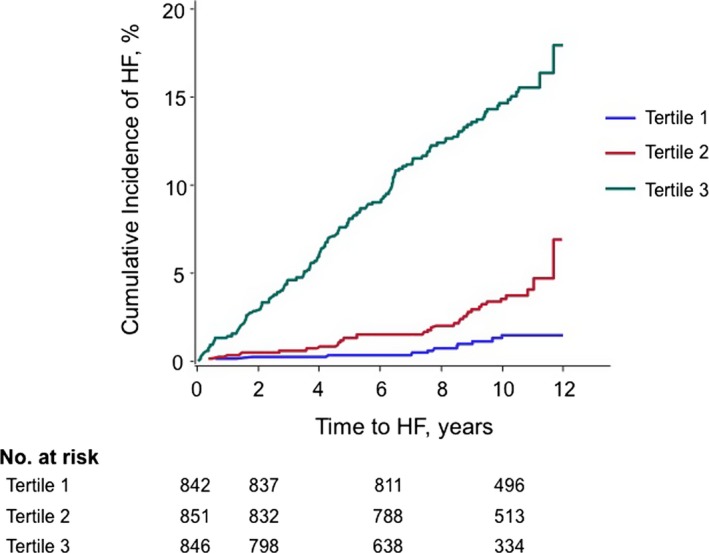
Methods and results: Framingham Study participants without clinical HF (n=2539, mean age 64 years, 56% women) underwent applanation tonometry to measure carotid-femoral pulse wave velocity (CFPWV), central pulse pressure, forward wave amplitude, and augmentation index. CFPWV was inverse-transformed to reduce heteroscedasticity and multiplied by -1 to restore effect direction (iCFPWV). Over 10.1 (range 0.04-12.9) years, 170 HF events developed. In multivariable-adjusted analyses, iCFPWV was associated with incident HF in a continuous, graded fashion (hazards ratio [HR] per SD unit [SDU] 1.29, 95% confidence interval [CI] 1.02-1.64, P=0.037). iCFPWV was associated with HF with reduced ejection fraction (HR=1.69/SDU, 95% CI 1.19-2.42, P=0.0037) in age- and sex-adjusted models, which was attenuated in multivariable-adjusted models (P=0.065). Central pulse pressure and forward wave amplitude were associated with HF in age- and sex-adjusted models (per SDU, HR=1.20, 95% CI 1.06-1.37, P=0.006, and HR=1.15, 95% CI 1.01-1.31, P=0.036, respectively), but not in multivariable-adjusted models (both P≥0.28). Augmentation index was not associated with HF risk (P≥0.19 in all models).
Conclusions: In our prospective investigation of a large community-based sample of middle-aged to elderly individuals, greater aortic stiffness (reflected by higher iCFPWV) was associated with increased risk of HF. Future studies may investigate the impact of modifying aortic stiffness in reducing the community burden of HF.
Keywords: aortic stiffness; epidemiology; heart failure; pressure pulsatility.
© 2015 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
Comment in
-
From Arterial Stiffness to Heart Failure: Still a Long Way to Go.J Am Heart Assoc. 2015 Nov 23;4(11):e002807. doi: 10.1161/JAHA.115.002807. J Am Heart Assoc. 2015. PMID: 26597156 Free PMC article. No abstract available.
References
-
- Alecu C, Gueguen R, Aubry C, Salvi P, Perret‐Guillaume C, Ducrocq X, Vespignani H, Benetos A. Determinants of arterial stiffness in an apparently healthy population over 60 years. J Hum Hypertens. 2006;20:749–756. - PubMed
-
- Mitchell GF, Guo CY, Benjamin EJ, Larson MG, Keyes MJ, Vita JA, Vasan RS, Levy D. Cross‐sectional correlates of increased aortic stiffness in the community: the Framingham Heart Study. Circulation. 2007;115:2628–2636. - PubMed
-
- Mattace‐Raso FU, van der Cammen TJ, Hofman A, van Popele NM, Bos ML, Schalekamp MA, Asmar R, Reneman RS, Hoeks AP, Breteler MM, Witteman JC. Arterial stiffness and risk of coronary heart disease and stroke: the Rotterdam Study. Circulation. 2006;113:657–663. - PubMed
-
- Sutton‐Tyrrell K, Najjar SS, Boudreau RM, Venkitachalam L, Kupelian V, Simonsick EM, Havlik R, Lakatta EG, Spurgeon H, Kritchevsky S, Pahor M, Bauer D, Newman A. Elevated aortic pulse wave velocity, a marker of arterial stiffness, predicts cardiovascular events in well‐functioning older adults. Circulation. 2005;111:3384–3390. - PubMed
Publication types
MeSH terms
Grants and funding
- HL107385/HL/NHLBI NIH HHS/United States
- HL080124/HL/NHLBI NIH HHS/United States
- R01 HL077447/HL/NHLBI NIH HHS/United States
- 6R01-NS-17950/NS/NINDS NIH HHS/United States
- HHSN268201500001I/HL/NHLBI NIH HHS/United States
- HL060040/HL/NHLBI NIH HHS/United States
- 1K23 HL118259/HL/NHLBI NIH HHS/United States
- N01-HC-25195/HC/NHLBI NIH HHS/United States
- HL070100/HL/NHLBI NIH HHS/United States
- HHSN268201500001C/HL/NHLBI NIH HHS/United States
- R01 HL107385/HL/NHLBI NIH HHS/United States
- AG028321/AG/NIA NIH HHS/United States
- HL077447/HL/NHLBI NIH HHS/United States
- HL076784/HL/NHLBI NIH HHS/United States
- HHSN268201500001I/HL/NHLBI NIH HHS/United States
- R01 HL118259/HL/NHLBI NIH HHS/United States
- HL071039/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
