

Liraglutide in Type 2 Diabetes Mellitus: Clinical Pharmacokinetics and Pharmacodynamics
- PMID: 26597252
- PMCID: PMC4875959
- DOI: 10.1007/s40262-015-0343-6
Liraglutide in Type 2 Diabetes Mellitus: Clinical Pharmacokinetics and Pharmacodynamics
Abstract
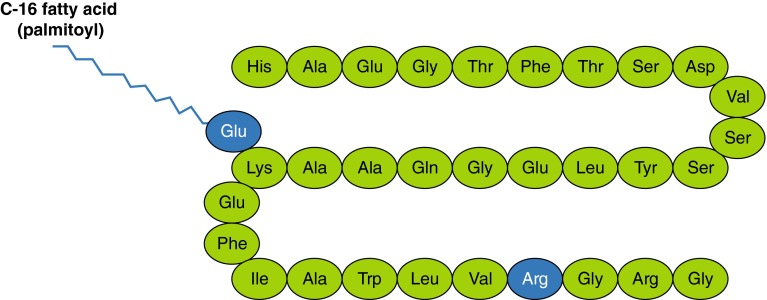
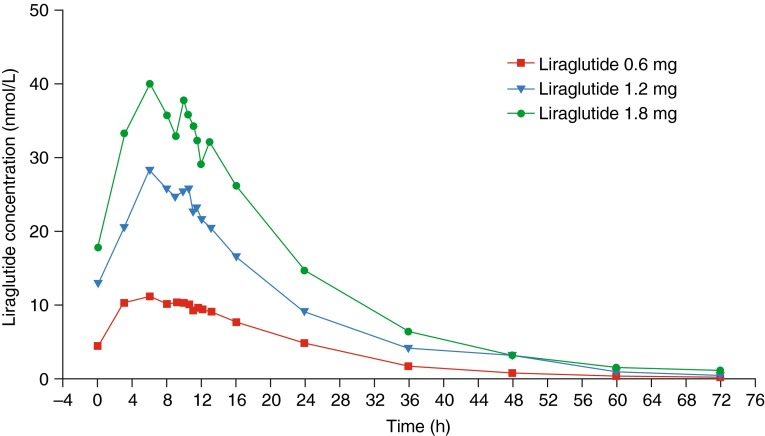
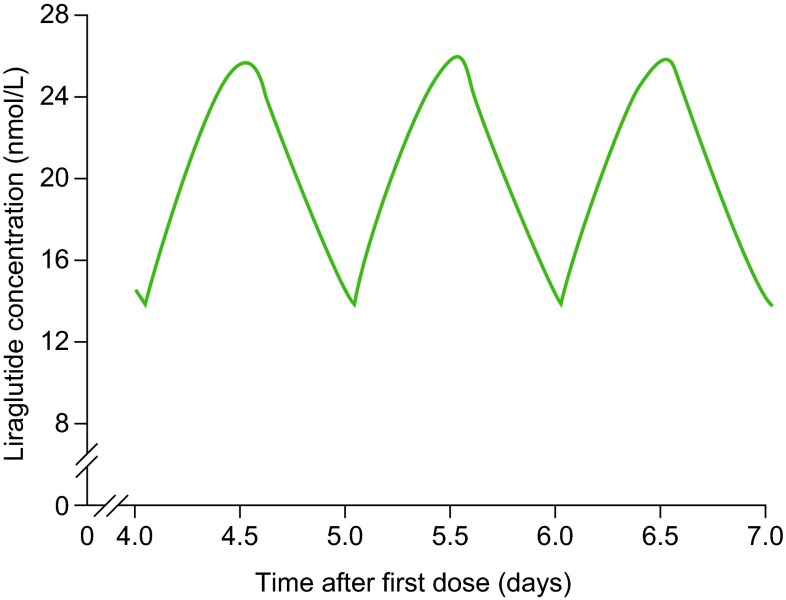
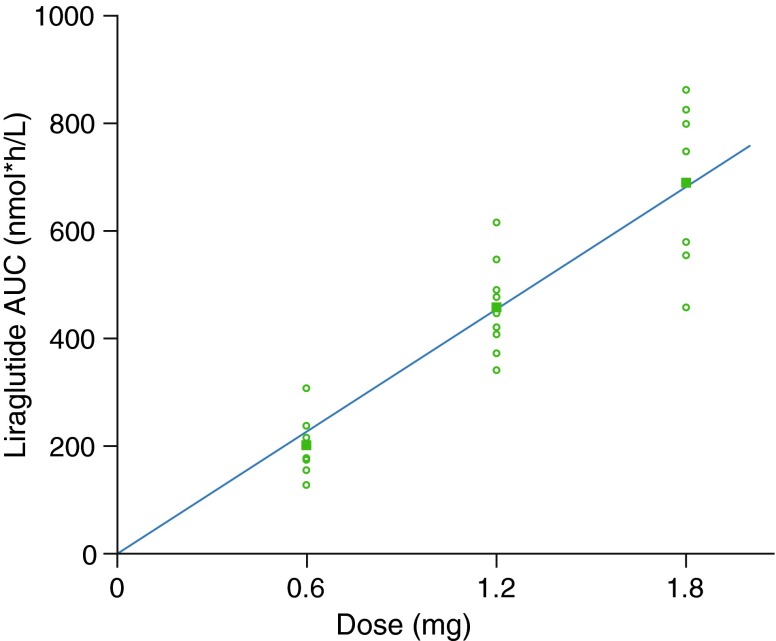
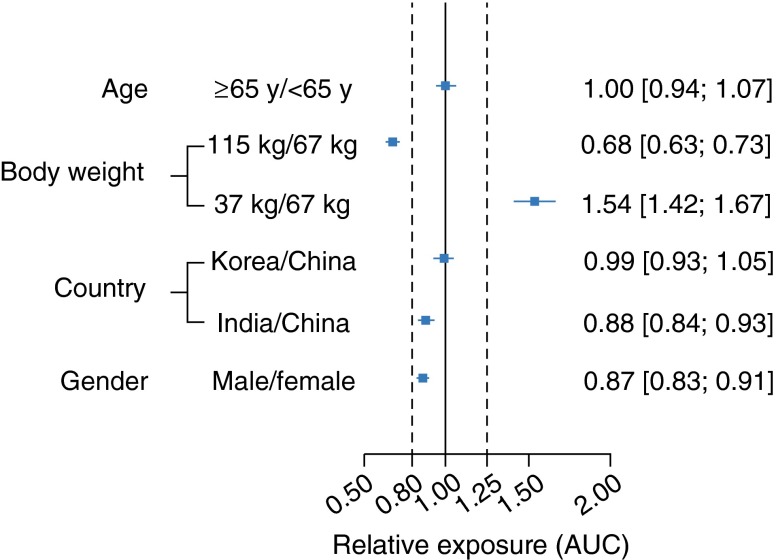
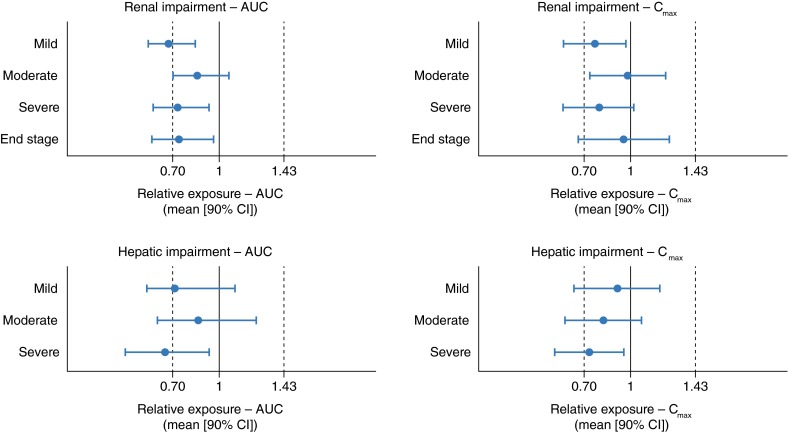
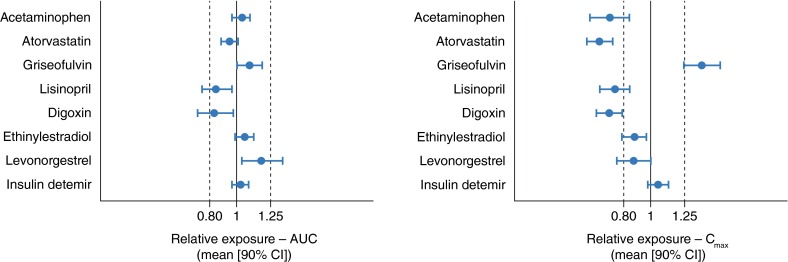
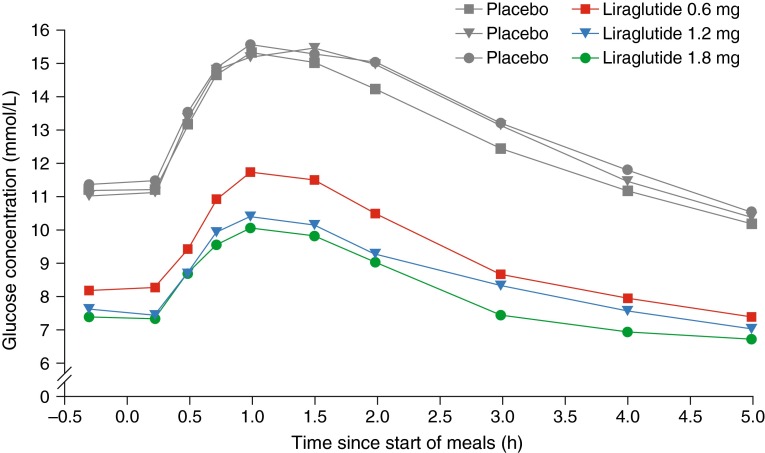
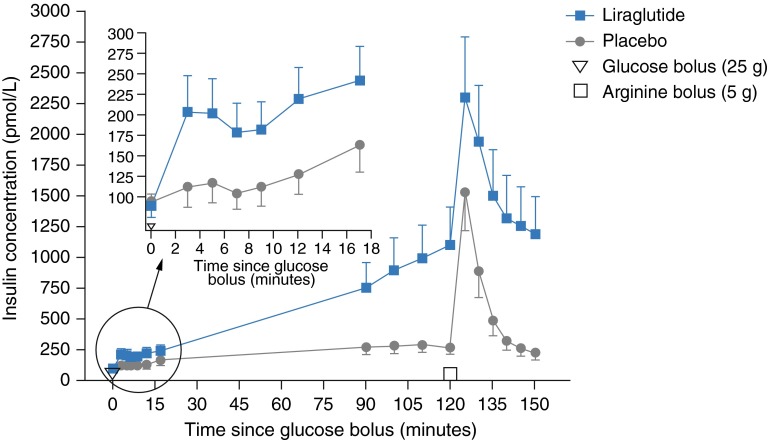
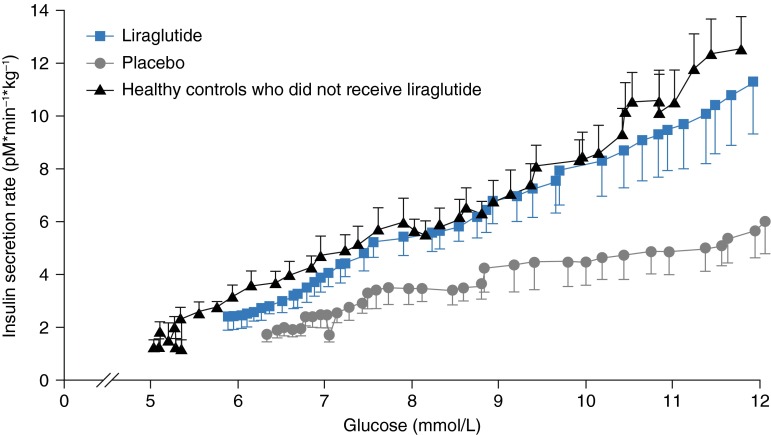
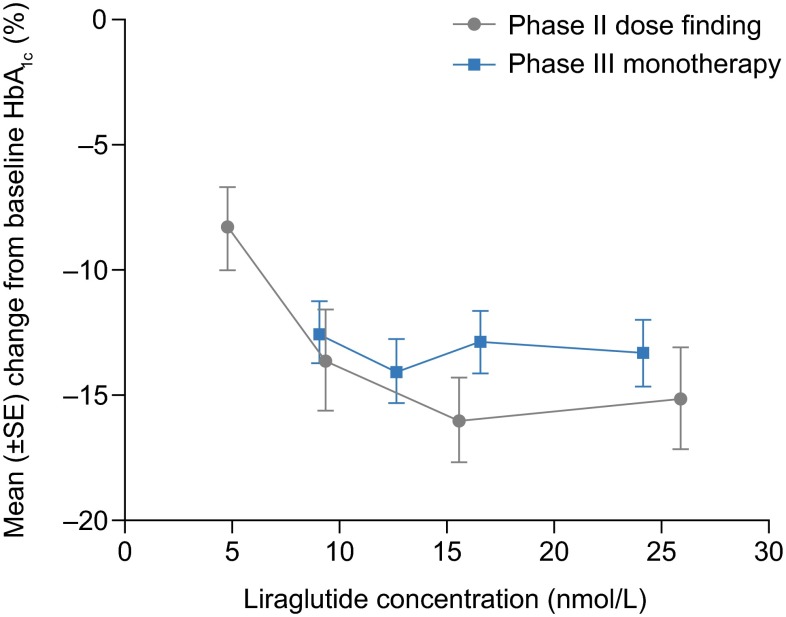
Liraglutide is an acylated glucagon-like peptide-1 analogue with 97 % amino acid homology with native glucagon-like peptide-1 and greatly protracted action. It is widely used for the treatment of type 2 diabetes mellitus, and administered by subcutaneous injection once daily. The pharmacokinetic properties of liraglutide enable 24-h exposure coverage, a requirement for 24-h glycaemic control with once-daily dosing. The mechanism of protraction relates to slowed release from the injection site, and a reduced elimination rate owing to metabolic stabilisation and reduced renal filtration. Drug exposure is largely independent of injection site, as well as age, race and ethnicity. Increasing body weight and male sex are associated with reduced concentrations, but there is substantial overlap between subgroups; therefore, dose escalation should be based on individual treatment outcome. Exposure is reduced with mild, moderate or severe renal or hepatic impairment. There are no clinically relevant changes in overall concentrations of various drugs (e.g. paracetamol, atorvastatin, griseofulvin, digoxin, lisinopril and oral combination contraceptives) when co-administered with liraglutide. Pharmacodynamic studies show multiple beneficial actions with liraglutide, including improved fasting and postprandial glycaemic control (mediated by increased insulin and reduced glucagon levels and minor delays in gastric emptying), reduced appetite and energy intake, and effects on postprandial lipid profiles. The counter-regulatory hormone response to hypoglycaemia is largely unaltered. The effects of liraglutide on insulin and glucagon secretion are glucose dependent, and hence the risk of hypoglycaemia is low. The pharmacokinetic and pharmacodynamic properties of liraglutide make it an important treatment option for many patients with type 2 diabetes.
Figures
References
-
- International Diabetes Federation. Diabetes atlas: sixth edition. 2014 update. http://www.idf.org/diabetesatlas. Accessed 24 Sep 2015.
-
- International Diabetes Federation. About diabetes. https://www.idf.org/about-diabetes. Accessed 23 Sep 2015.
-
- Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M, et al. Management of hyperglycaemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) Diabetologia. 2012;55:1577–1596. doi: 10.1007/s00125-012-2534-0. - DOI - PubMed
-
- International Diabetes Federation Clinical Guidelines Task Force. Global guideline for type 2 diabetes. 2012. http://www.idf.org/sites/default/files/IDF-Guideline-for-Type-2-Diabetes.... Accessed 23 Sep 2015.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
