

Breath-hold imaging of the coronary arteries using Quiescent-Interval Slice-Selective (QISS) magnetic resonance angiography: pilot study at 1.5 Tesla and 3 Tesla
- PMID: 26597281
- PMCID: PMC4655490
- DOI: 10.1186/s12968-015-0205-2
Breath-hold imaging of the coronary arteries using Quiescent-Interval Slice-Selective (QISS) magnetic resonance angiography: pilot study at 1.5 Tesla and 3 Tesla
Abstract
Background: Coronary magnetic resonance angiography (MRA) is usually obtained with a free-breathing navigator-gated 3D acquisition. Our aim was to develop an alternative breath-hold approach that would allow the coronary arteries to be evaluated in a much shorter time and without risk of degradation by respiratory motion artifacts. For this purpose, we implemented a breath-hold, non-contrast-enhanced, quiescent-interval slice-selective (QISS) 2D technique. Sequence performance was compared at 1.5 and 3 Tesla using both radial and Cartesian k-space trajectories.
Methods: The left coronary circulation was imaged in six healthy subjects and two patients with coronary artery disease. Breath-hold QISS was compared with T2-prepared 2D balanced steady-state free-precession (bSSFP) and free-breathing, navigator-gated 3D bSSFP.
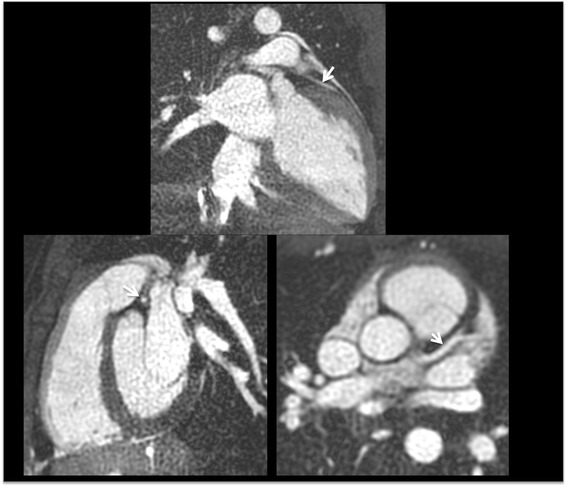
Results: Approximately 10 2.1-mm thick slices were acquired in a single ~20-s breath-hold using two-shot QISS. QISS contrast-to-noise ratio (CNR) was 1.5-fold higher at 3 Tesla than at 1.5 Tesla. Cartesian QISS provided the best coronary-to-myocardium CNR, whereas radial QISS provided the sharpest coronary images. QISS image quality exceeded that of free-breathing 3D coronary MRA with few artifacts at either field strength. Compared with T2-prepared 2D bSSFP, multi-slice capability was not restricted by the specific absorption rate at 3 Tesla and pericardial fluid signal was better suppressed. In addition to depicting the coronary arteries, QISS could image intra-cardiac structures, pericardium, and the aortic root in arbitrary slice orientations.
Conclusions: Breath-hold QISS is a simple, versatile, and time-efficient method for coronary MRA that provides excellent image quality at both 1.5 and 3 Tesla. Image quality exceeded that of free-breathing, navigator-gated 3D MRA in a much shorter scan time. QISS also allowed rapid multi-slice bright-blood, diastolic phase imaging of the heart, which may have complementary value to multi-phase cine imaging. We conclude that, with further clinical validation, QISS might provide an efficient alternative to commonly used free-breathing coronary MRA techniques.
Figures






References
-
- In the original publication (Magn Reson Med 2010;63:951–958), the QISS acronym stood for “quiescent-interval single shot”. However, we have modified the acronym to stand for “quiescent-interval slice-selective” in order to more flexibly encompass more recent implementations of the technique for carotid and coronary MRA.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
