

Acid-Base Homeostasis
- PMID: 26597304
- PMCID: PMC4670772
- DOI: 10.2215/CJN.07400715
Acid-Base Homeostasis
Abstract
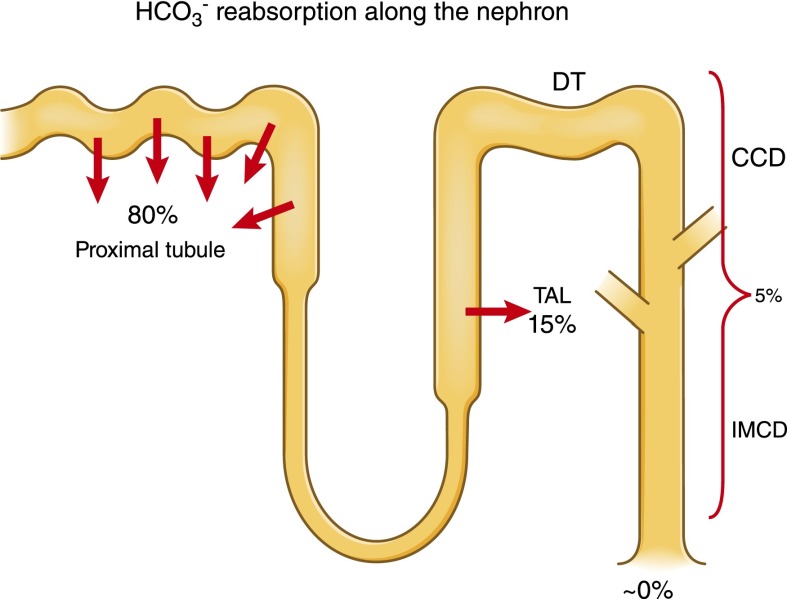
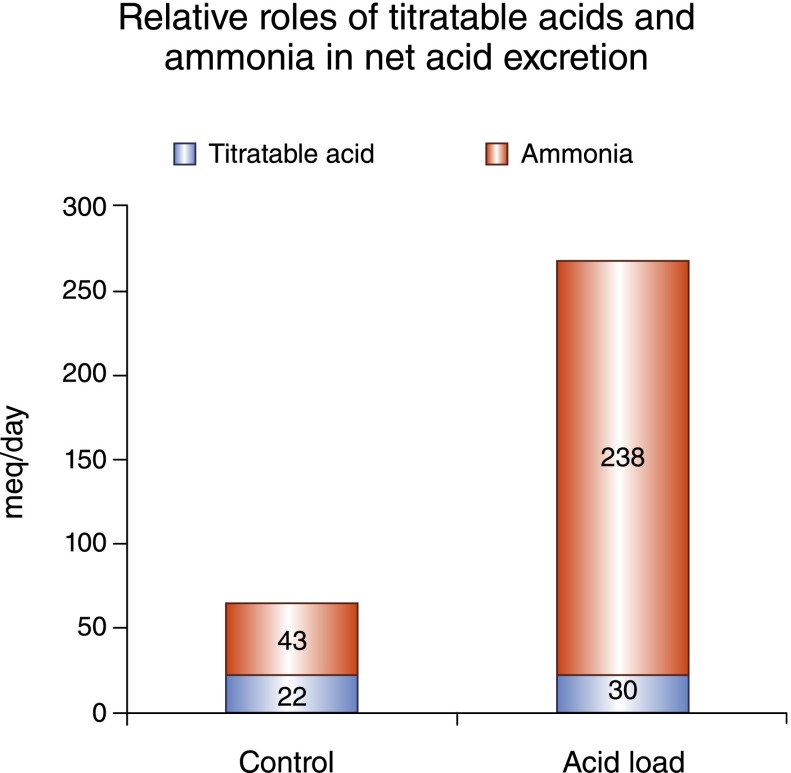
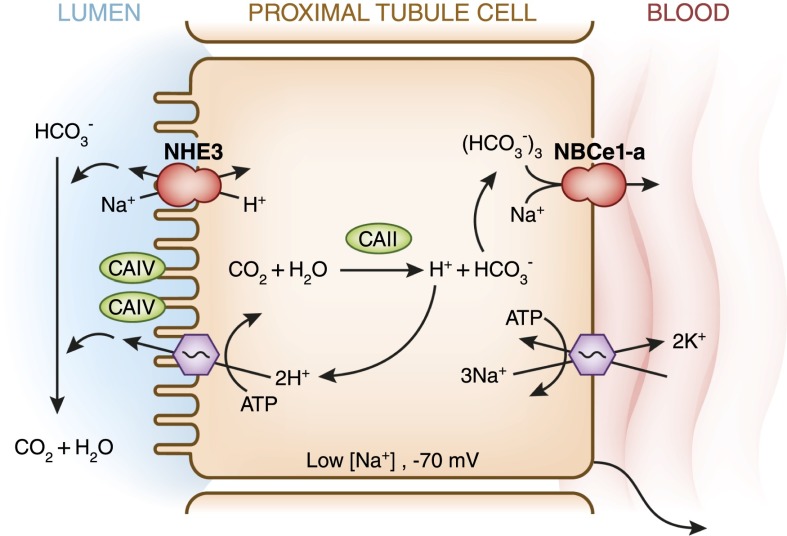
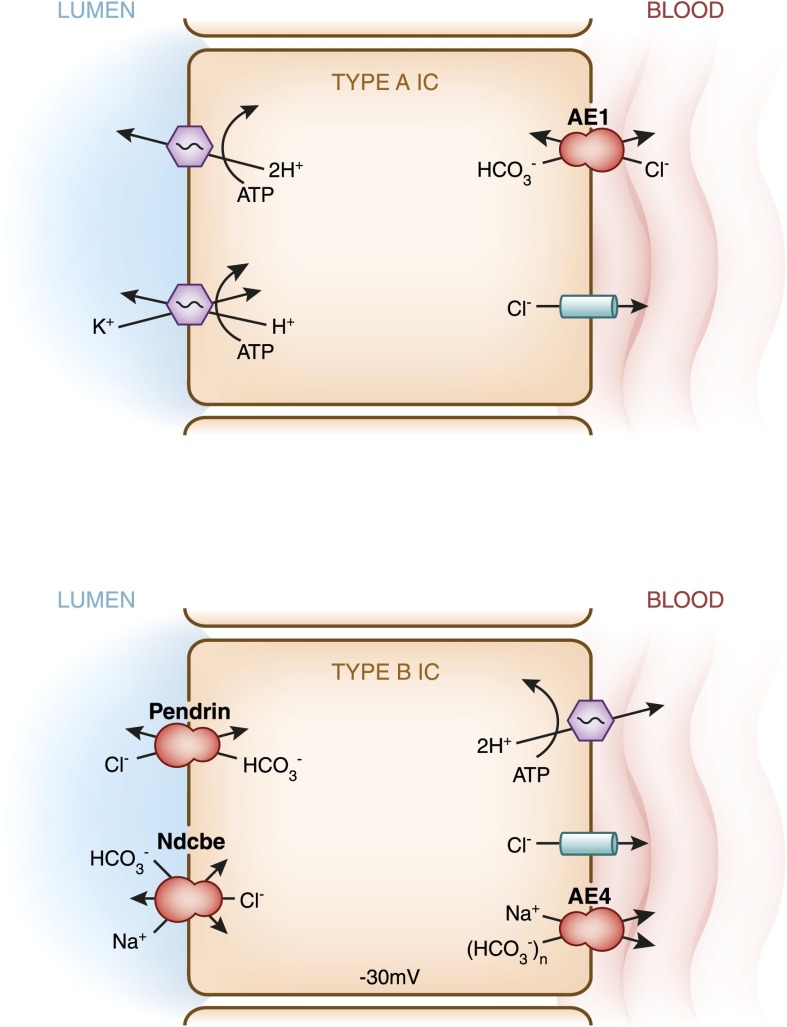
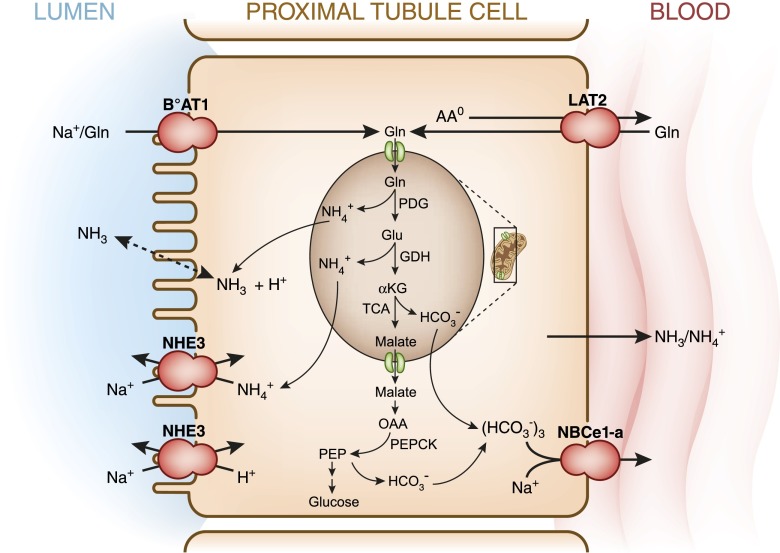
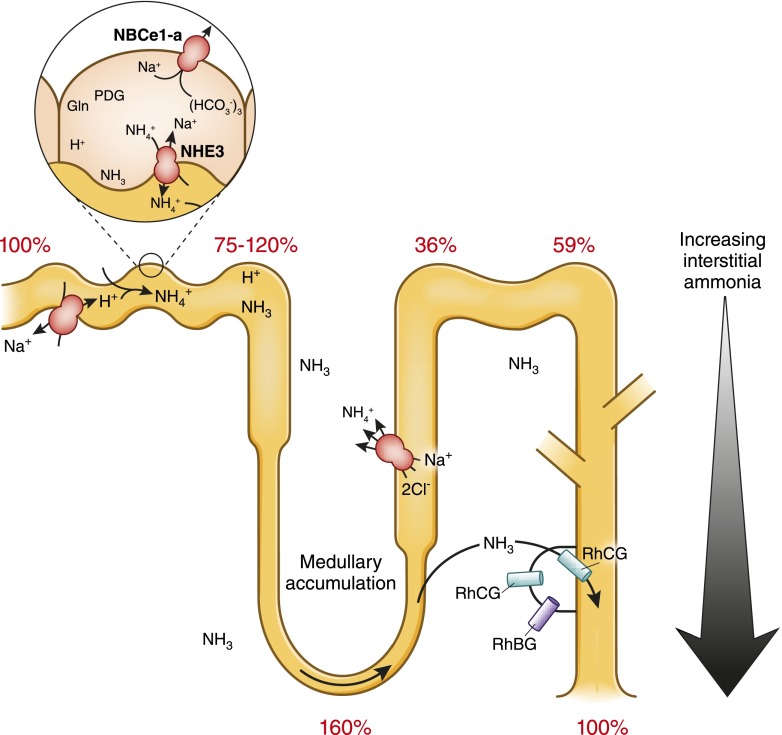
Acid-base homeostasis and pH regulation are critical for both normal physiology and cell metabolism and function. The importance of this regulation is evidenced by a variety of physiologic derangements that occur when plasma pH is either high or low. The kidneys have the predominant role in regulating the systemic bicarbonate concentration and hence, the metabolic component of acid-base balance. This function of the kidneys has two components: reabsorption of virtually all of the filtered HCO3(-) and production of new bicarbonate to replace that consumed by normal or pathologic acids. This production or generation of new HCO3(-) is done by net acid excretion. Under normal conditions, approximately one-third to one-half of net acid excretion by the kidneys is in the form of titratable acid. The other one-half to two-thirds is the excretion of ammonium. The capacity to excrete ammonium under conditions of acid loads is quantitatively much greater than the capacity to increase titratable acid. Multiple, often redundant pathways and processes exist to regulate these renal functions. Derangements in acid-base homeostasis, however, are common in clinical medicine and can often be related to the systems involved in acid-base transport in the kidneys.
Keywords: acid-base equilibrium; acid-base homeostasis; acidosis; bone density; chronic; homeostasis; kidney; nephrolithiasis; pH regulation; renal insufficiency; renal physiology.
Copyright © 2015 by the American Society of Nephrology.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
