

Temporal trends in the systemic inflammatory response syndrome, sepsis, and medical coding of sepsis
- PMID: 26597871
- PMCID: PMC4657245
- DOI: 10.1186/s12871-015-0148-z
Temporal trends in the systemic inflammatory response syndrome, sepsis, and medical coding of sepsis
Abstract
Background: Recent reports using administrative claims data suggest the incidence of community- and hospital-onset sepsis is increasing. Whether this reflects changing epidemiology, more effective diagnostic methods, or changes in physician documentation and medical coding practices is unclear.
Methods: We performed a temporal-trend study from 2008 to 2012 using administrative claims data and patient-level clinical data of adult patients admitted to Barnes-Jewish Hospital in St. Louis, Missouri. Temporal-trend and annual percent change were estimated using regression models with autoregressive integrated moving average errors.
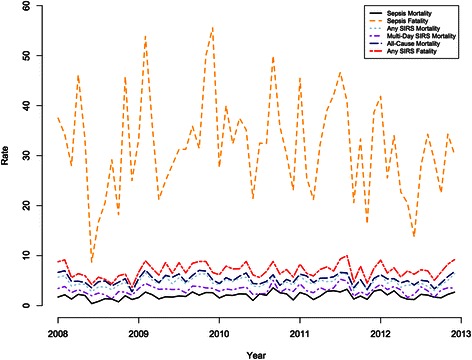
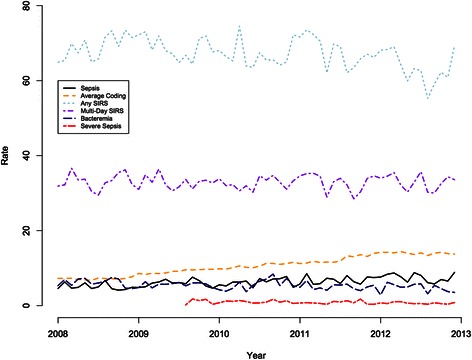
Results: We analyzed 62,261 inpatient admissions during the 5-year study period. 'Any SIRS' (i.e., SIRS on a single calendar day during the hospitalization) and 'multi-day SIRS' (i.e., SIRS on 3 or more calendar days), which both use patient-level data, and medical coding for sepsis (i.e., ICD-9-CM discharge diagnosis codes 995.91, 995.92, or 785.52) were present in 35.3 %, 17.3 %, and 3.3 % of admissions, respectively. The incidence of admissions coded for sepsis increased 9.7 % (95 % CI: 6.1, 13.4) per year, while the patient data-defined events of 'any SIRS' decreased by 1.8 % (95 % CI: -3.2, -0.5) and 'multi-day SIRS' did not change significantly over the study period. Clinically-defined sepsis (defined as SIRS plus bacteremia) and severe sepsis (defined as SIRS plus hypotension and bacteremia) decreased at statistically significant rates of 5.7 % (95 % CI: -9.0, -2.4) and 8.6 % (95 % CI: -4.4, -12.6) annually. All-cause mortality, SIRS mortality, and SIRS and clinically-defined sepsis case fatality did not change significantly during the study period. Sepsis mortality, based on ICD-9-CM codes, however, increased by 8.8 % (95 % CI: 1.9, 16.2) annually.
Conclusions: The incidence of sepsis, defined by ICD-9-CM codes, and sepsis mortality increased steadily without a concomitant increase in SIRS or clinically-defined sepsis. Our results highlight the need to develop strategies to integrate clinical patient-level data with administrative data to draw more accurate conclusions about the epidemiology of sepsis.
Figures
Comment in
-
Codifying healthcare--big data and the issue of misclassification.BMC Anesthesiol. 2015 Dec 15;15:179. doi: 10.1186/s12871-015-0165-y. BMC Anesthesiol. 2015. PMID: 26667619 Free PMC article.
References
-
- Patient safety indicators #4: technical specifications. Death rate among surgical inpatients with serious treatable complications [version 4.4]. AHRQ quality indicators 2012; March:9, 79.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
