

Dipeptidyl Peptidase 4 Distribution in the Human Respiratory Tract: Implications for the Middle East Respiratory Syndrome
- PMID: 26597880
- PMCID: PMC4715219
- DOI: 10.1016/j.ajpath.2015.09.014
Dipeptidyl Peptidase 4 Distribution in the Human Respiratory Tract: Implications for the Middle East Respiratory Syndrome
Abstract
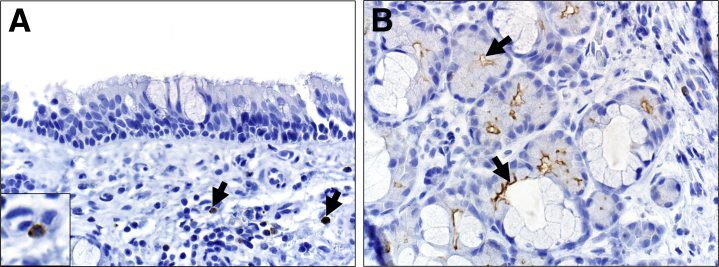
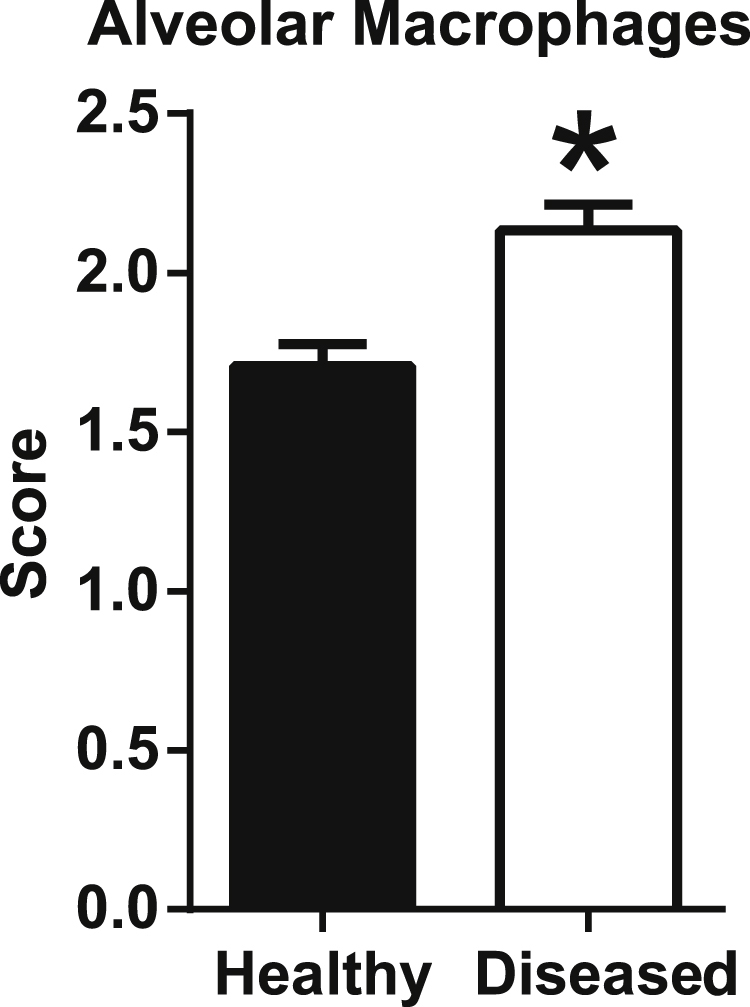
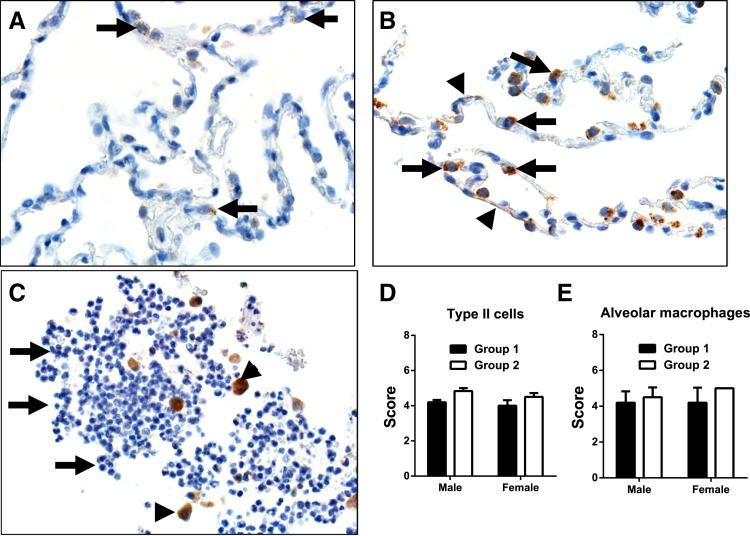
Dipeptidyl peptidase 4 (DPP4, CD26), a type II transmembrane ectopeptidase, is the receptor for the Middle Eastern respiratory syndrome coronavirus (MERS-CoV). MERS emerged in 2012 and has a high mortality associated with severe lung disease. A lack of autopsy studies from MERS fatalities has hindered understanding of MERS-CoV pathogenesis. We investigated the spatial and cellular localization of DPP4 to evaluate an association MERS clinical disease. DPP4 was rarely detected in the surface epithelium from nasal cavity to conducting airways with a slightly increased incidence in distal airways. DPP4 was also found in a subset of mononuclear leukocytes and in serous cells of submucosal glands. In the parenchyma, DPP4 was found principally in type I and II cells and alveolar macrophages and was also detected in vascular endothelium (eg, lymphatics) and pleural mesothelia. Patients with chronic lung disease, such as chronic obstructive pulmonary disease and cystic fibrosis, exhibited increased DPP4 immunostaining in alveolar epithelia (type I and II cells) and alveolar macrophages with similar trends in reactive mesothelia. This finding suggests that preexisting pulmonary disease could increase MERS-CoV receptor abundance and predispose individuals to MERS morbidity and mortality, which is consistent with current clinical observations. We speculate that the preferential spatial localization of DPP4 in alveolar regions may explain why MERS is characterized by lower respiratory tract disease.
Copyright © 2016 American Society for Investigative Pathology. Published by Elsevier Inc. All rights reserved.
Figures



References
-
- Zaki A.M., van Boheemen S., Bestebroer T.M., Osterhaus A.D., Fouchier R.A. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012;367:1814–1820. - PubMed
-
- Arabi Y.M., Arifi A.A., Balkhy H.H., Najm H., Aldawood A.S., Ghabashi A., Hawa H., Alothman A., Khaldi A., Al Raiy B. Clinical course and outcomes of critically ill patients with Middle East respiratory syndrome coronavirus infection. Ann Intern Med. 2014;160:389–397. - PubMed
-
- Kapoor M., Pringle K., Kumar A., Dearth S., Liu L., Lovchik J., Perez O., Pontones P., Richards S., Yeadon-Fagbohun J., Breakwell L., Chea N., Cohen N.J., Schneider E., Erdman D., Haynes L., Pallansch M., Tao Y., Tong S., Gerber S., Swerdlow D., Feikin D.R. Clinical and laboratory findings of the first imported case of Middle East respiratory syndrome coronavirus to the United States. Clin Infect Dis. 2014;59:1511–1518. - PMC - PubMed
-
- Saad M., Omrani A.S., Baig K., Bahloul A., Elzein F., Matin M.A., Selim M.A., Al Mutairi M., Al Nakhli D., Al Aidaroos A.Y., Al Sherbeeni N., Al-Khashan H.I., Memish Z.A., Albarrak A.M. Clinical aspects and outcomes of 70 patients with Middle East respiratory syndrome coronavirus infection: a single-center experience in Saudi Arabia. Int J Infect Dis. 2014;29:301–306. - PMC - PubMed
-
- Assiri A., McGeer A., Perl T.M., Price C.S., Al Rabeeah A.A., Cummings D.A., Alabdullatif Z.N., Assad M., Almulhim A., Makhdoom H., Madani H., Alhakeem R., Al-Tawfiq J.A., Cotten M., Watson S.J., Kellam P., Zumla A.I., Memish Z.A., Team KM-CI Hospital outbreak of Middle East respiratory syndrome coronavirus. N Engl J Med. 2013;369:407–416. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
