

Effects of passive leg raising and volume expansion on mean systemic pressure and venous return in shock in humans
- PMID: 26597901
- PMCID: PMC4657233
- DOI: 10.1186/s13054-015-1115-2
Effects of passive leg raising and volume expansion on mean systemic pressure and venous return in shock in humans
Abstract
Introduction: The aim of this study was to assess how mean systemic pressure (Psm) and resistance to venous return (Rvr) behave during passive leg raising (PLR) in cases of fluid responsiveness and fluid unresponsiveness.
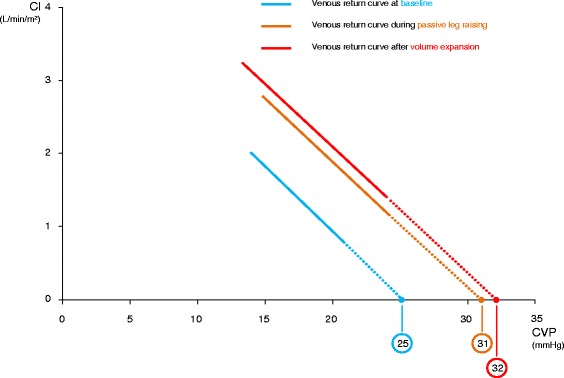
Method: In 30 patients with an acute circulatory failure, in order to estimate the venous return curve, we constructed the regression line between pairs of cardiac index (CI) and central venous pressure (CVP). Values were measured during end-inspiratory and end-expiratory ventilatory occlusions performed at two levels of positive end-expiratory pressure. The x-axis intercept was used to estimate Psm and the inverse of the slope to quantify Rvr. These measurements were obtained at baseline, during PLR and after fluid infusion. Patients in whom fluid infusion increased CI by more than 15 % were defined as "fluid-responders".
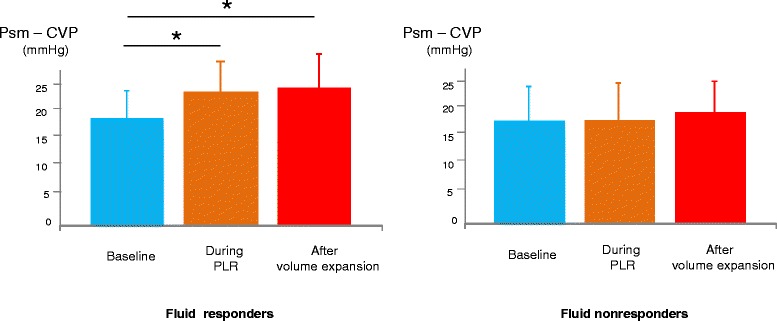
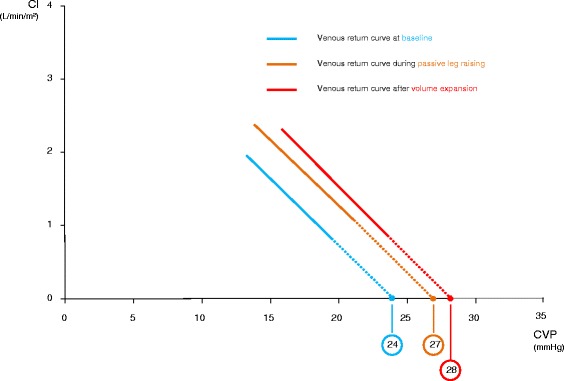
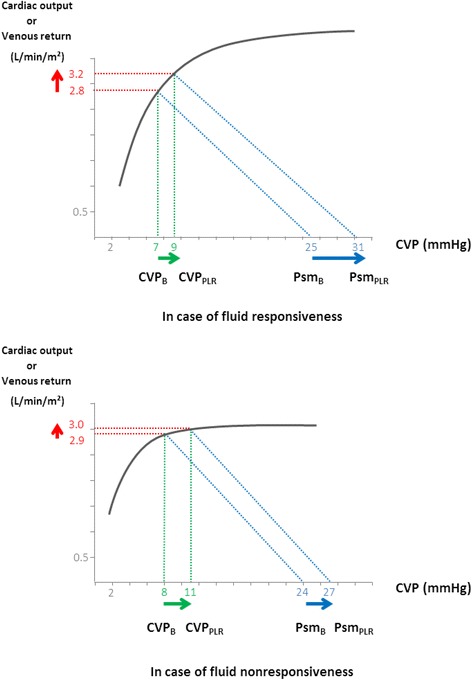
Results: In fluid-responders (n = 15), CVP and Psm significantly increased (from 7 ± 3 to 9 ± 4 mmHg and from 25 ± 13 to 31 ± 13 mmHg, respectively) during PLR. The Psm-CVP gradient significantly increased by 20 ± 30 % while Rvr did not change significantly during PLR. In fluid-nonresponders, CVP and Psm increased significantly but the Psm-CVP gradient did not change significantly during PLR. PLR did not change the intra-abdominal pressure in the whole population (14 ± 6 mmHg before vs. 13 ± 5 mmHg during PLR, p = 0.26) and in patients with intra-abdominal hypertension at baseline (17 ± 4 mmHg before vs. 16 ± 4 mmHg during PLR, p = 0.14). In the latter group, PLR increased Psm from 22 ± 11 to 27 ± 10 mmHg (p <0.01) and did not change Rvr (5.1 ± 2.6 to 5.2 ± 3 mmHg/min/m(2)/mL, p = 0.71). In fluid-responders, Psm, CVP and the Psm-CVP gradient significantly increased during fluid infusion while the Rvr did not change. In fluid-nonresponders, CVP and Psm increased significantly during fluid infusion while the Psm-CVP gradient and Rvr did not change.
Conclusion: PLR significantly increased Psm without modifying Rvr. This was also the case in patients with intra-abdominal hypertension. In case of fluid responsiveness, PLR increased venous return by increasing Psm to a larger extent than CVP. In patients with fluid unresponsiveness, PLR increased Psm but did not change the Psm-CVP gradient. Fluid infusion induced similar effects on Psm and Rvr.
Figures
References
-
- Guyton AC, Lindsey AW, Abernathy B, Richardson T. Venous return at various right atrial pressures and the normal venous return curve. Am J Physiol. 1957;189:609–15. - PubMed
-
- Schipke JD, Heusch G, Sanii AP et al Static filling 1 pressure in patients during induced ventricular fibrillation. Am J Physiol Heart Circ Physiol. 2003; 285:H2510–2515. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
