

Intensive care at the end of life in patients dying due to non-cancer chronic diseases versus cancer: a nationwide study in Denmark
- PMID: 26597917
- PMCID: PMC4657209
- DOI: 10.1186/s13054-015-1124-1
Intensive care at the end of life in patients dying due to non-cancer chronic diseases versus cancer: a nationwide study in Denmark
Abstract
Introduction: It is unknown to what extent use of palliative care and focus on proactive planning of end-of-life (EOL) care among cancer patients is also reflected by less use of intensive care. We aimed to examine the use of intensive care in the EOL in patients dying as a result of non-cancer diseases compared with patients dying due to cancer.
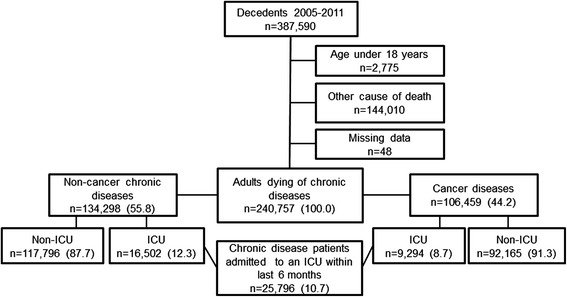
Methods: We conducted a nationwide follow-up study among 240,757 adults dying as a result of either non-cancer chronic disease or cancer in Denmark between 2005 and 2011. Using the Danish Intensive Care Database, we identified all admissions and treatments in intensive care units (ICU) during the patients' last 6 months before death. We used prevalence ratios (aPRs) adjusted for age, sex, comorbidity, marital status and residential region to compare the 6-month prevalence of ICU admissions as well as treatment with invasive mechanical ventilation (MV), non-invasive ventilation (NIV), renal replacement therapy (RRT) and inotropes and/or vasopressors. In addition, length of ICU stay and death during ICU admission were compared among non-cancer and cancer patients dying between 2009 and 2011.
Results: Overall 12.3 % of non-cancer patients were admitted to an ICU within their last 6 months of life, compared with 8.7 % of cancer patients. The overall aPR for ICU admission was 2.11 [95 % confidence interval (CI) 1.98-2.24] for non-cancer patients compared with cancer patients and varied widely within the non-cancer patients (patients with dementia, aPR 0.19, 95 % CI 0.17-0.21; patients with chronic obstructive lung disease, aPR 3.19, 95 % CI 2.97-3.41). The overall aPRs for treatment among non-cancer patients compared with cancer patients were 1.40 (95 % CI 1.35-1.46) for MV, 1.62 (95 % CI 1.50-1.76) for NIV, 1.19 (95 % CI 1.07-1.31) for RRT and 1.05 (95 % CI 0.87-1.28) for inotropes and/or vasopressors. No difference in admission length was observed. Non-cancer patients had an increased risk of dying in an ICU (aPR 1.23, 95 % CI 0.99-1.54) compared with cancer patients.
Conclusions: Overall, patients dying as a result of non-cancer diseases were twice as likely to be admitted to ICUs at the EOL as patients dying due to cancer. Further studies are warranted to explore whether this difference in use of intensive care reflects an unmet need of palliative care, poor communication about the EOL or lack of prognostic tools for terminally ill non-cancer patients.
Figures

References
-
- World Health Organization. Cancer. Fact sheet 297 [updated February 2015]. http://www.who.int/mediacentre/factsheets/fs297/en/. Accessed 9 Nov 2015.
-
- World Health Organization. The top 10 causes of death. Fact sheet 310 [updated May 2014]. http://www.who.int/mediacentre/factsheets/fs310/en/. Accessed 9 Nov 2015.
-
- Goodman DC, Esty AR, Fisher ES, Chang CH. Trends and variation in end-of-life care for Medicare beneficiaries with severe chronic illness: a report of the Dartmouth Atlas Project. Hanover, NH: The Dartmouth Institute for Health Policy & Clinical Practice; 12 Apr 2011. http://www.dartmouthatlas.org/downloads/reports/EOL_Trend_Report_0411.pdf. Accessed 9 Nov 2015. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
