

Resuscitative endovascular balloon occlusion of the aorta (REBOA): a population based gap analysis of trauma patients in England and Wales
- PMID: 26598631
- PMCID: PMC4717355
- DOI: 10.1136/emermed-2015-205217
Resuscitative endovascular balloon occlusion of the aorta (REBOA): a population based gap analysis of trauma patients in England and Wales
Abstract
Introduction: Non-compressible torso haemorrhage (NCTH) carries a high mortality in trauma as many patients exsanguinate prior to definitive haemorrhage control. Resuscitative endovascular balloon occlusion of the aorta (REBOA) is an adjunct that has the potential to bridge patients to definitive haemostasis. However, the proportion of trauma patients in whom REBOA may be utilised is unknown.
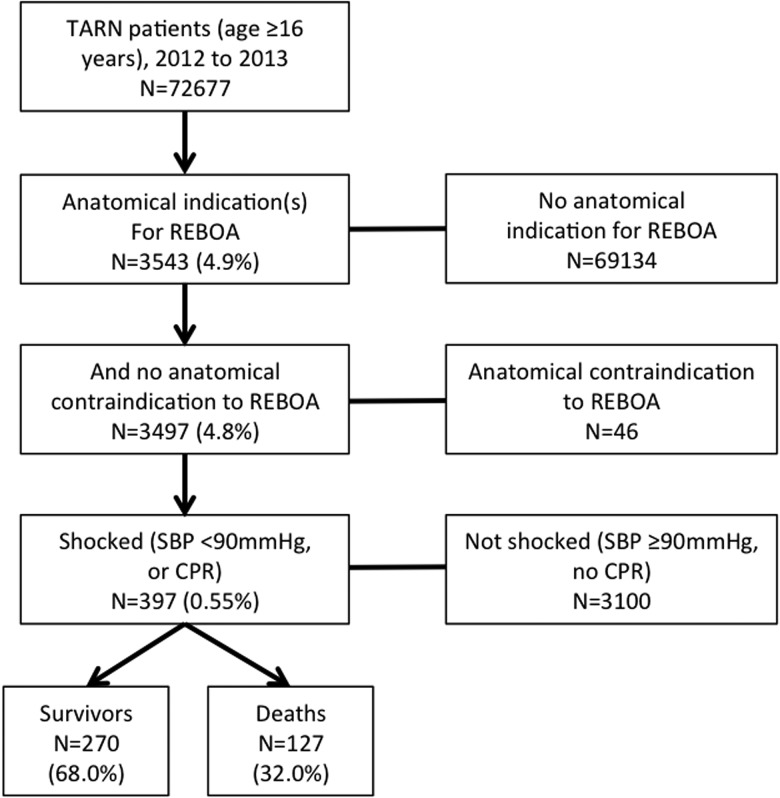
Methods: We conducted a population based analysis of 2012-2013 Trauma Audit and Research Network (TARN) data. We identified the number of patients in whom REBOA may have been utilised, defined by an Abbreviated Injury Scale score ≥3 to abdominal solid organs, abdominal or pelvic vasculature, pelvic fracture with ring disruption or proximal traumatic lower limb amputation, together with a systolic blood pressure <90 mm Hg. Patients with non-compressible haemorrhage in the mediastinum, axilla, face or neck were excluded.
Results: During 2012-2013, 72 677 adult trauma patients admitted to hospitals in England and Wales were identified. 397 patients had an indication(s) and no contraindications for REBOA with evidence of haemorrhagic shock: 69% men, median age 43 years and median Injury Severity Score 32. Overall mortality was 32%. Major trauma centres (MTCs) received the highest concentration of potential REBOA patients, and would be anticipated to receive a patient in whom REBOA may be utilised every 95 days, increasing to every 46 days in the 10 MTCs with the highest attendance of this injury type.
Conclusions: This TARN database analysis has identified a small group of severely injured, resource intensive patients with a highly lethal injury that is theoretically amenable to REBOA. The highest density of these patients is seen at MTCs, and as such a planned evaluation of REBOA should be further considered in these hospitals.
Keywords: Trauma; Trauma, abdomen; Trauma, epidemiology; Trauma, majot trauma management; resuscitation.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures

References
-
- National Audit Office. Major trauma care in England. London: The Stationery Office; 2010.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous