

Adjuvant Chemotherapy Use and Health Care Costs After Introduction of Genomic Testing in Breast Cancer
- PMID: 26598749
- PMCID: PMC5321084
- DOI: 10.1200/JCO.2015.61.9023
Adjuvant Chemotherapy Use and Health Care Costs After Introduction of Genomic Testing in Breast Cancer
Abstract
Purpose: We assessed the associations between the 21-gene recurrence score assay (RS) receipt, subsequent chemotherapy use, and medical expenditures among patients with early-stage breast cancer.
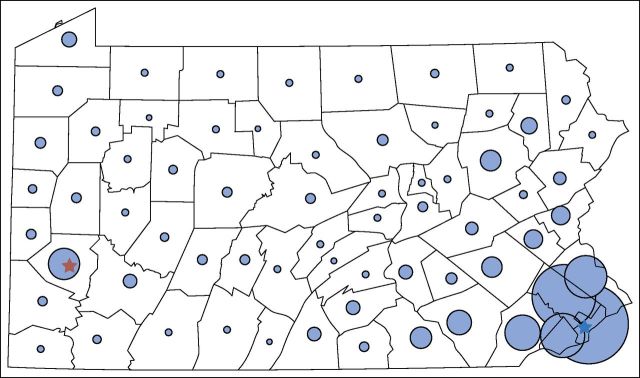
Patients and methods: Data from the Pennsylvania Cancer Registry were used to assemble a retrospective cohort of women with early-stage breast cancer from 2007 to 2010 who underwent initial surgical treatment. These data were merged with administrative claims from the 12-month periods before and after diagnosis to identify comorbidities, treatments, and expenditures (n = 7,287). Propensity score-weighted regression models were estimated to identify the effects of RS receipt on chemotherapy use and medical spending in the year after diagnosis.
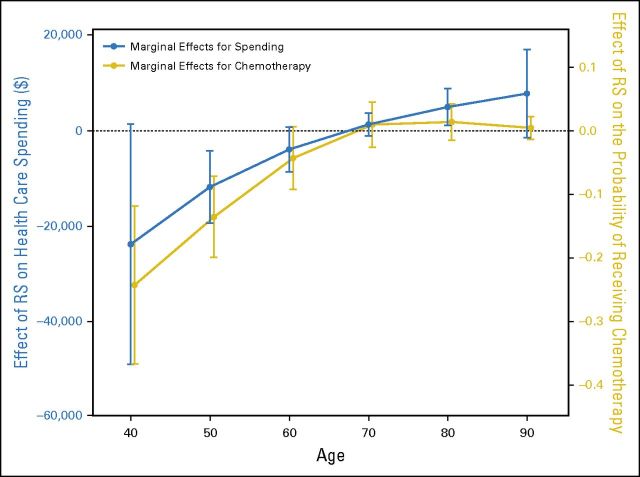
Results: The associations between RS receipt and outcomes varied markedly by patient age. RS use was associated with lower chemotherapy use among women younger than 55 (19.2% lower; 95% CI, 10.6 to 27.9). RS use was associated with higher chemotherapy use among women 75 to 84 years old (5.7% higher; 95% CI, 0.4 to 11.0). RS receipt was associated with lower adjusted 1-year medical spending among women younger than 55 ($15,333 lower; 95% CI, $2,841 to $27,824) and with higher spending among women who were 75 to 84 years old ($3,489 higher; 95% CI, $857 to $6,122).
Conclusion: RS receipt was associated with reduced use of adjuvant chemotherapy and lower health care spending among women with breast cancer who were younger than 55. Conversely, among women 75 and older, RS testing was associated with a modest increase in chemotherapy use and slightly higher spending. From a population perspective, the impact of RS testing on breast cancer treatment and health care costs is much greater in younger women.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at
Figures
References
-
- Fisher B, Jeong JH, Bryant J, et al. National Surgical Adjuvant Breast and Bowel Project randomised clinical trials Treatment of lymph-node-negative, oestrogen-receptor-positive breast cancer: Long-term findings from National Surgical Adjuvant Breast and Bowel Project randomised clinical trials. Lancet. 2004;364:858–868. - PubMed
-
- Fisher B, Dignam J, Wolmark N, et al. Tamoxifen and chemotherapy for lymph node-negative, estrogen receptor-positive breast cancer. J Natl Cancer Inst. 1997;89:1673–1682. - PubMed
-
- Azim HA, Jr, de Azambuja E, Colozza M, et al. Long-term toxic effects of adjuvant chemotherapy in breast cancer. Ann Oncol. 2011;22:1939–1947. - PubMed
-
- Nguyen MT, Stessin A, Nagar H, et al. Impact of oncotype DX recurrence score in the management of breast cancer cases. Clin Breast Cancer. 2014;14:182–190. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
