

Long-term outcomes after randomization to buprenorphine/naloxone versus methadone in a multi-site trial
- PMID: 26599131
- PMCID: PMC4801718
- DOI: 10.1111/add.13238
Long-term outcomes after randomization to buprenorphine/naloxone versus methadone in a multi-site trial
Abstract
Aims: To compare long-term outcomes among participants randomized to buprenorphine or methadone.
Design, setting and participants: Follow-up was conducted in 2011-14 of 1080 opioid-dependent participants entering seven opioid treatment programs in the United States between 2006 and 2009 and randomized (within each program) to receive open-label buprenorphine/naloxone or methadone for up to 24 weeks; 795 participants completed in-person interviews (~74% follow-up interview rate) covering on average 4.5 years.
Measurements: Outcomes were indicated by mortality and opioid use. Covariates included demographics, site, cocaine use and treatment experiences.
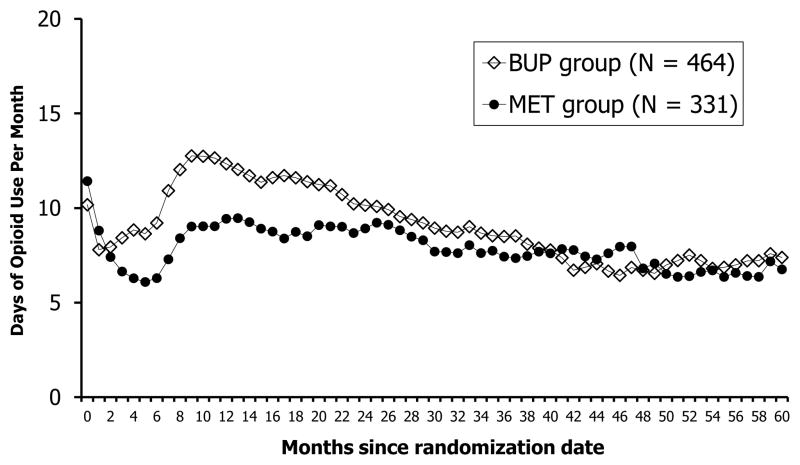
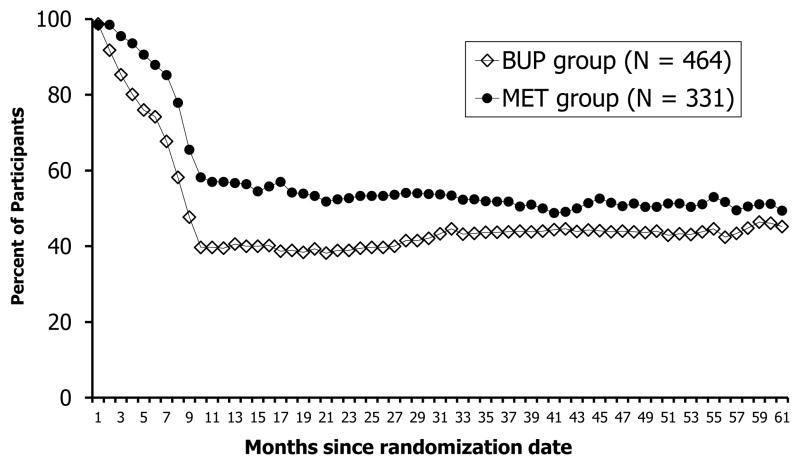
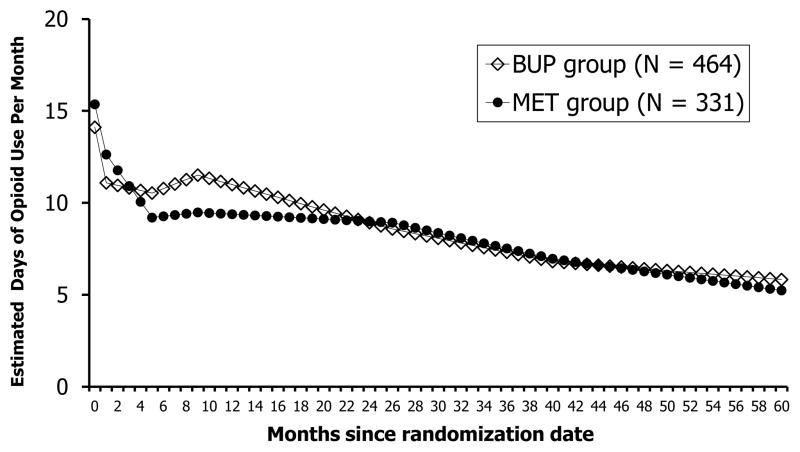
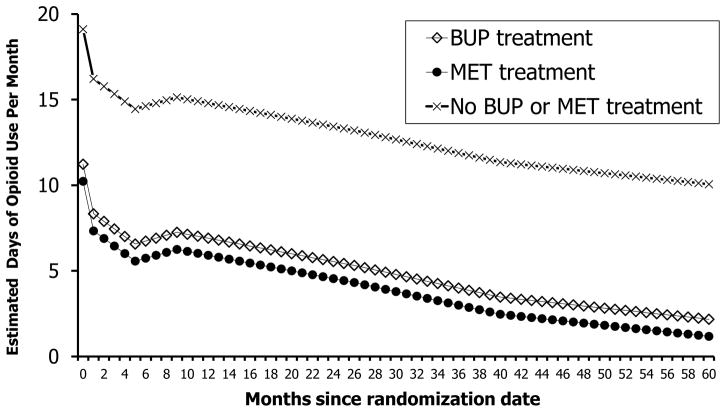
Findings: Mortality was not different between the two randomized conditions, with 23 (3.6%) of 630 participants randomized to buprenorphine having died versus 26 (5.8%) of 450 participants randomized to methadone. Opioid use at follow-up was higher among participants randomized to buprenorphine relative to methadone [42.8 versus 31.7% positive opioid urine specimens, P < 0.01, effect size (h) = 0.23 (0.09, 0.38); 5.8 days versus 4.4 days of past 30-day heroin use, P < 0.05, effect size (d) = 0.14 (0.00, 0.28)]. Opioid use during the follow-up period by randomization condition was also significant (F(7,39,600) = 3.16; P < 0.001) due mainly to less treatment participation among participants randomized to buprenorphine than methadone. Less opioid use was associated with both buprenorphine and methadone treatment (relative to no treatment); no difference was found between the two treatments. Individuals who are white or used cocaine at baseline responded better to methadone than to buprenorphine.
Conclusions: There are few differences in long-term outcomes between buprenorphine and methadone treatment for opioid dependence, and treatment with each medication is associated with a strong reduction in opioid use.
Keywords: Buprenorphine; longitudinal; methadone; mortality; opioid dependence; opioid use; outcomes.
© 2015 Society for the Study of Addiction.
Conflict of interest statement
Declaration of Interest: Authors disclosing relevant financial interests, activities, relationships, and affiliations are:
Walter Ling: Consultant to Reckitt Benckiser Pharmaceuticals.
Andrew Saxon: Consultant to Reckitt Benckiser Pharmaceuticals, advisory board member for Alkermes, Inc., and receive royalties as an editor for UpToDate.
George Woody: Consultant to Reckitt Benckiser Pharmaceuticals.
All other authors report no financial or other possible conflicts of interest.
Figures
References
-
- Hser YI, Evans E, Grella C, Ling W, Anglin D. Long-term course of opioid addiction. Harv Rev Psychiatry. 2015;23:76–89. - PubMed
-
- NIH Consensus Statement. Effective medical treatment of opiate addiction. National Consensus Development Panel on Effective Medical Treatment of Opiate Addiction. JAMA. 1998;280:1936–1943. - PubMed
-
- Bell J, Trinh L, Butler B, Randall D, Rubin G. Comparing retention in treatment and mortality in people after initial entry to methadone and buprenorphine treatment. Addiction. 2009;104:1193–1200. - PubMed
-
- Connock M, Juarez-Garcia A, Jowett S, et al. Methadone and buprenorphine for the management of opioid dependence: a systematic review and economic evaluation. Health Technol Assess. 2007;11:1–171. iii–iv. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 DA13038/DA/NIDA NIH HHS/United States
- U10 DA13043/DA/NIDA NIH HHS/United States
- U10 DA 015815/DA/NIDA NIH HHS/United States
- P30 AI028697/AI/NIAID NIH HHS/United States
- UG1 DA013035/DA/NIDA NIH HHS/United States
- U10 DA013043/DA/NIDA NIH HHS/United States
- U10 DA015815/DA/NIDA NIH HHS/United States
- U10 DA01714/DA/NIDA NIH HHS/United States
- UG1 DA013714/DA/NIDA NIH HHS/United States
- U10 DA013045/DA/NIDA NIH HHS/United States
- P30DA016383/DA/NIDA NIH HHS/United States
- P30 DA016383/DA/NIDA NIH HHS/United States
- U10 DA013038/DA/NIDA NIH HHS/United States
- U10 DA13045/DA/NIDA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
