

Gliomas: Motexafin Gadolinium-enhanced Molecular MR Imaging and Optical Imaging for Potential Intraoperative Delineation of Tumor Margins
- PMID: 26599802
- PMCID: PMC4851136
- DOI: 10.1148/radiol.2015150895
Gliomas: Motexafin Gadolinium-enhanced Molecular MR Imaging and Optical Imaging for Potential Intraoperative Delineation of Tumor Margins
Abstract
Purpose: To investigate the possibility of using motexafin gadolinium (MGd)-enhanced molecular magnetic resonance (MR) imaging and optical imaging to identify the true margins of gliomas.
Materials and methods: The animal protocol was approved by the institutional animal care and use committee. Thirty-six Sprague-Dawley rats with gliomas were randomized into six groups of six rats. Five groups were euthanized 15, 30, 60, 120, and 240 minutes after intravenous administration of 6 mg/kg of MGd, while one group received only saline solution as a control group. After craniotomy, optical imaging and T1-weighted MR imaging were performed to identify the tumor margins. One-way analysis of variance was used to compare optical photon intensity and MR imaging signal-to-noise ratios. Histologic analysis was performed to confirm the intracellular uptake of MGd by tumor cells and to correlate the tumor margins delineated on both optical and MR images.
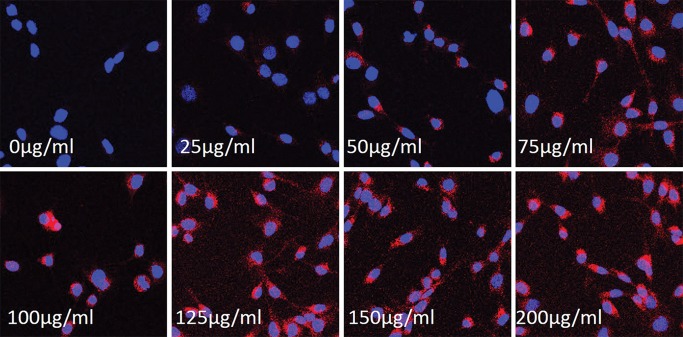
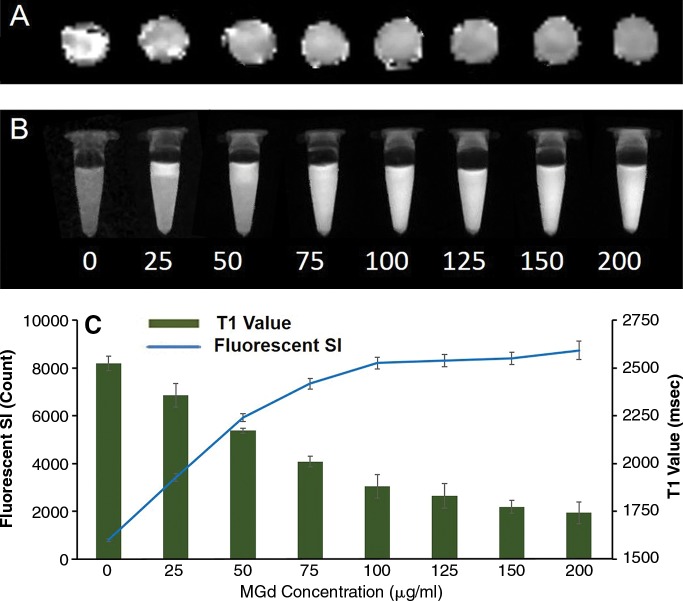
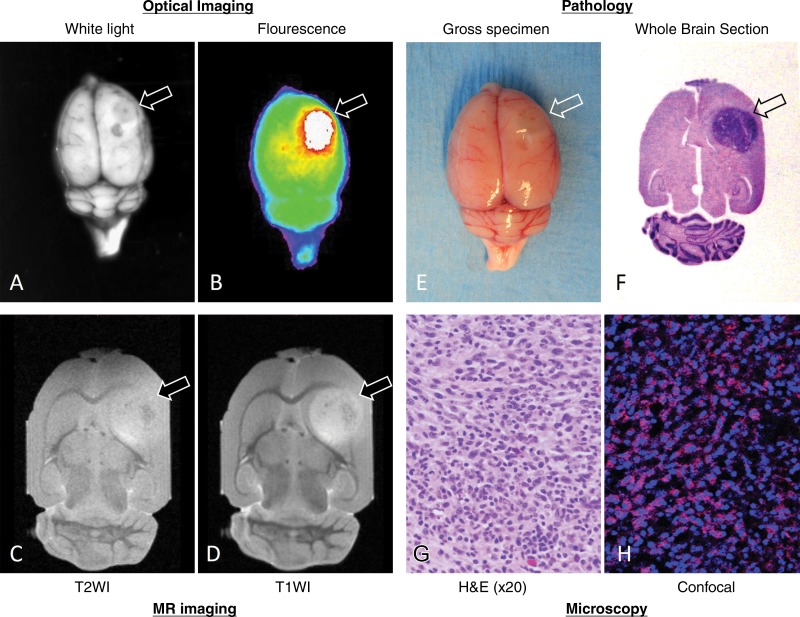
Results: Both optical imaging and T1-weighted MR imaging showed tumor margins. The highest optical photon intensity (2.6 × 10(8) photons per second per mm(2) ± 2.3 × 10(7); analysis of variance, P < .001) and MR signal-to-noise ratio (77.61 ± 2.52; analysis of variance, P = .006) were reached at 15-30 minutes after administration of MGd, with continued tumor visibility at 2-4 hours. Examination with confocal microscopy allowed confirmation that the fluorescence of optical images and MR imaging T1 enhancement exclusively originated from MGd that accumulated in the cytoplasm of tumor cells.
Conclusion: MGd-enhanced optical and MR imaging can allow determination of glioma tumor margins at the optimal time of 15-120 minutes after administration of MGd. Clinical application of these results may allow complete removal of gliomas in a hybrid surgical setting in which intraoperative optical and MR imaging are available.
(©) RSNA, 2015.
Figures



References
-
- Meyer MA. Malignant gliomas in adults. N Engl J Med 2008;359(17):1850; author reply 1850. - PubMed
-
- Stummer W, Pichlmeier U, Meinel T, et al. . Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre phase III trial. Lancet Oncol 2006;7(5):392–401. - PubMed
-
- Colditz MJ, Jeffree RL. Aminolevulinic acid (ALA)-protoporphyrin IX fluorescence guided tumour resection. Part 1: clinical, radiological and pathological studies. J Clin Neurosci 2012;19(11):1471–1474. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
