

Cost-Utility Analysis of Mycophenolate Mofetil versus Azathioprine Based Regimens for Maintenance Therapy of Proliferative Lupus Nephritis
- PMID: 26600951
- PMCID: PMC4639665
- DOI: 10.1155/2015/917567
Cost-Utility Analysis of Mycophenolate Mofetil versus Azathioprine Based Regimens for Maintenance Therapy of Proliferative Lupus Nephritis
Abstract
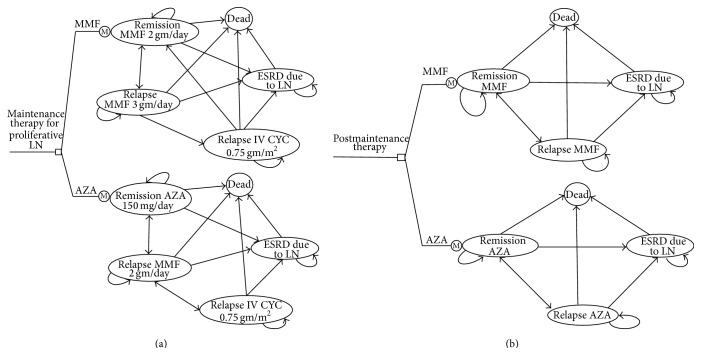
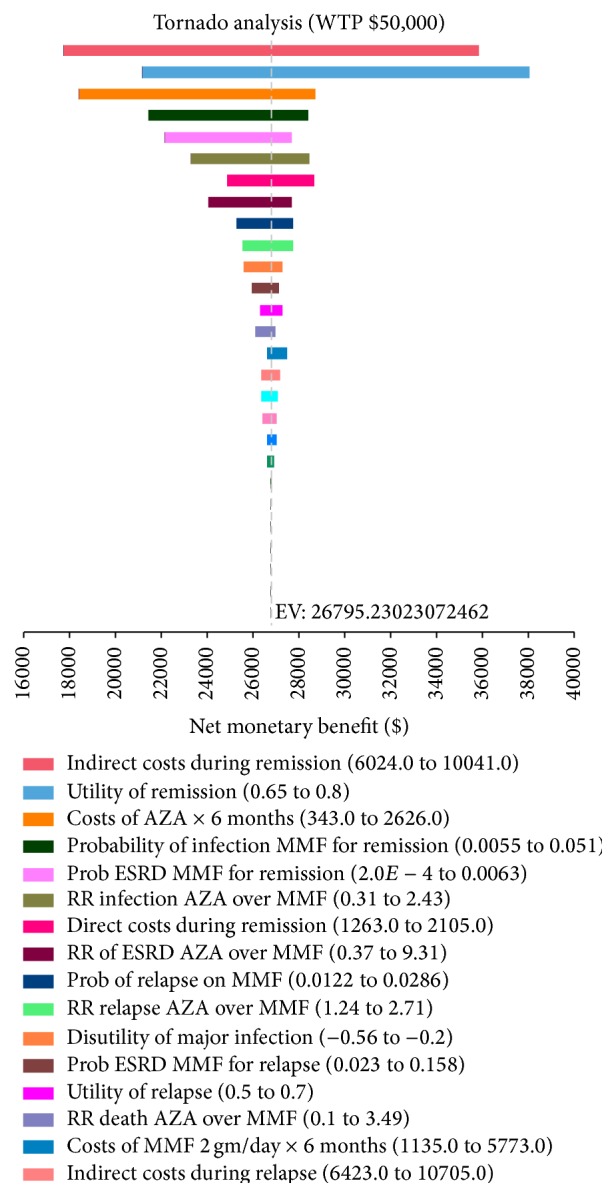
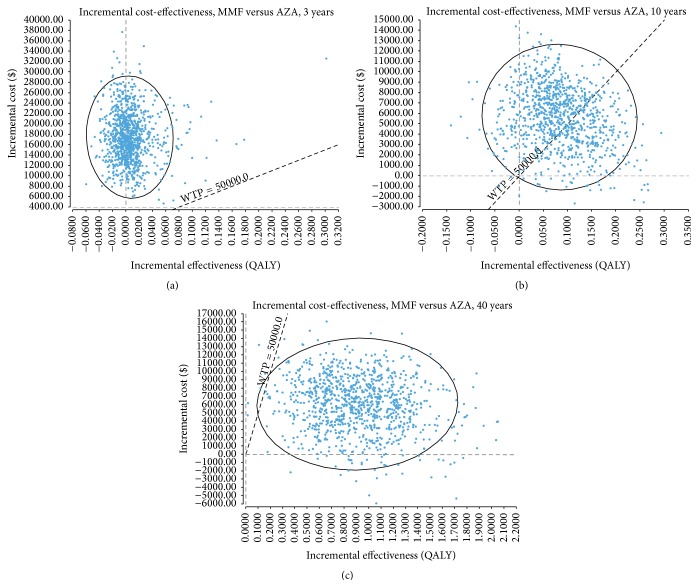
Background/Aims. We aimed to examine the cost-effectiveness of mycophenolate mofetil (MMF) and azathioprine (AZA) as maintenance therapy for patients with Class III and Class IV lupus nephritis (LN), from a United States (US) perspective. Methods. Using a Markov model, we conducted a cost-utility analysis from a societal perspective over a lifetime horizon. The modeled population comprised patients with proliferative LN who received maintenance therapy with MMF (2 gm/day) versus AZA (150 mg/day) for 3 years. Risk estimates of clinical events were based on a Cochrane meta-analysis while costs and utilities were retrieved from other published sources. Outcome measures included costs, quality-adjusted life-years (QALY), incremental cost-effectiveness ratios (ICER), and net monetary benefit. Results. The base-case model showed that, compared with AZA strategy, the ICER for MMF was $2,630,592/QALY at 3 years. Over the patients' lifetime, however, the ICER of MMF compared to AZA was $6,454/QALY. Overall, the ICER results from various sensitivity and subgroup analyses did not alter the conclusions of the model simulation. Conclusions. In the short term, an AZA-based regimen confers greater value than MMF for the maintenance therapy of proliferative LN. From a lifelong perspective, however, MMF is cost-effective compared to AZA.
Figures
References
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Glomerulonephritis Work Group. KDIGO clinical practice guideline for glomerulonephritis. Kidney International Supplements. 2012;2(2):139–274. doi: 10.1038/kisup.2012.9. - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources
