

Effects of lanreotide Autogel primary therapy on symptoms and quality-of-life in acromegaly: data from the PRIMARYS study
- PMID: 26603536
- PMCID: PMC4799252
- DOI: 10.1007/s11102-015-0693-y
Effects of lanreotide Autogel primary therapy on symptoms and quality-of-life in acromegaly: data from the PRIMARYS study
Abstract
Purpose: To evaluate the effects of lanreotide Autogel on patient-reported outcomes and association with biochemical control, using PRIMARYS data.
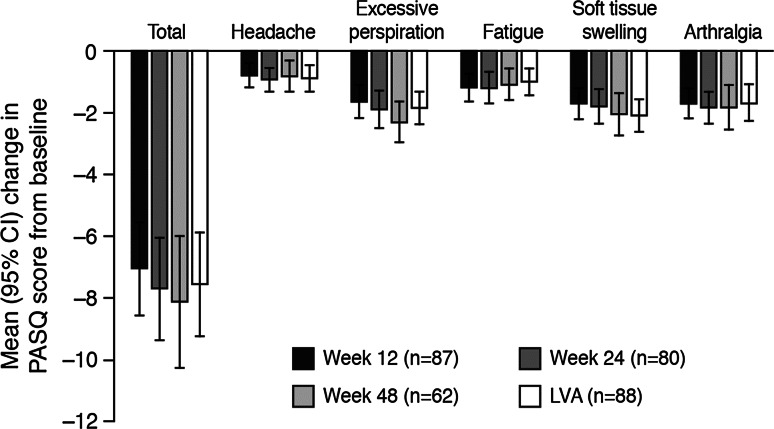
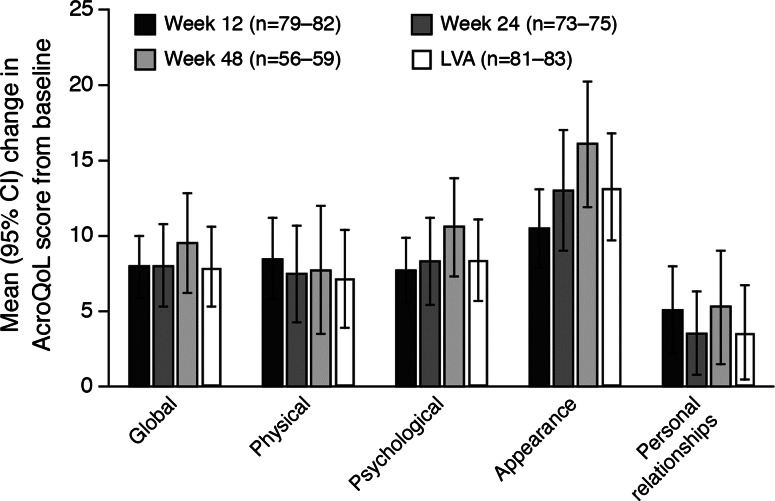
Methods: PRIMARYS was a 1-year, open-label study of lanreotide Autogel (Depot in USA) 120 mg every 4 weeks in 90 treatment-naïve patients with acromegaly. Symptoms were assessed using Patient-assessed Acromegaly Symptom Questionnaire (PASQ) and health-related quality of life (HRQoL) using the AcroQoL questionnaire. Correlations between PASQ and AcroQoL scores, and between PASQ/AcroQoL and growth hormone (GH)/insulin-like growth factor-1 (IGF-1) levels were also evaluated (post hoc).
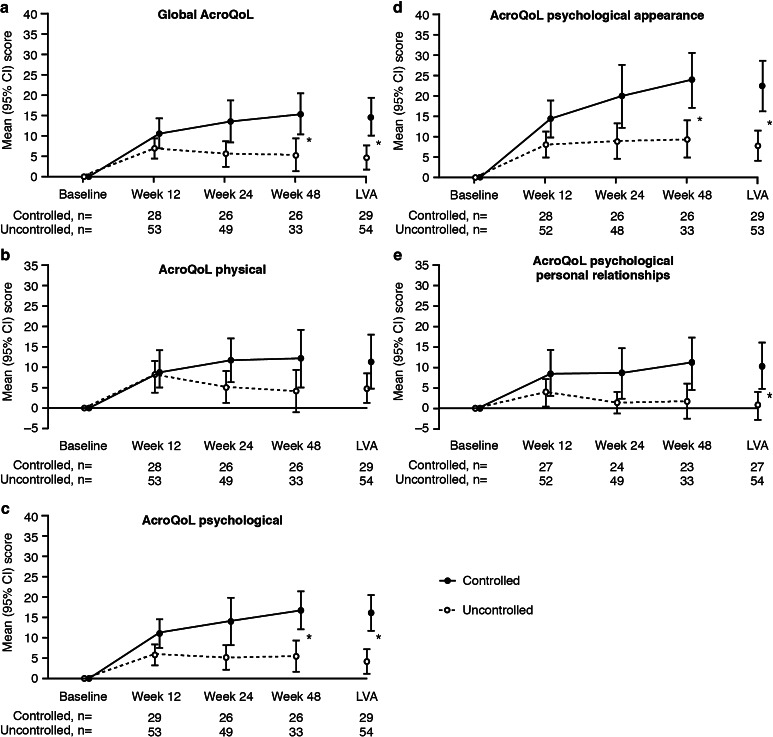
Results: Acromegaly symptoms and HRQoL significantly improved from week 12 to week 48, with modest correlations at week 48 between PASQ total score (R = -0.55, p < 0.0001) and AcroQoL global and physical scores (R = -0.67, p < 0.0001). Approximately 60% of patients achieved a minimal important difference (MID; improvement >50% of baseline standard deviation) in PASQ total score and >40% achieved a MID in AcroQoL global score (post hoc). Changes in PASQ scores were similar in biochemically controlled (GH levels ≤2.5 μg/L and normal IGF-1 levels) and uncontrolled groups, while changes in global and psychological AcroQoL scores were greater in the controlled group. There was no correlation between changes in PASQ or AcroQoL scores and changes in GH or IGF-1 levels.
Conclusions: Primary treatment with lanreotide Autogel over 1 year was associated with rapid and sustained improvements in clinical signs and symptoms and HRQoL in patients with acromegaly. Improvements in HRQoL, but not symptoms, were greater in those achieving biochemical control (ClinicalTrials.gov: NCT00690898; EudraCT: 2007-000155-34).
Keywords: Acromegaly; Lanreotide Autogel; Quality of life; Symptoms.
Figures
References
-
- Giustina A, Chanson P, Kleinberg D, Bronstein MD, Clemmons DR, Klibanski A, van der Lely AJ, Strasburger CJ, Lamberts SW, Ho KK, Casanueva FF, Melmed S, Acromegaly Consensus Group Expert consensus document: a consensus on the medical treatment of acromegaly. Nat Rev Endocrinol. 2014;10:243–248. doi: 10.1038/nrendo.2014.21. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
