

Epidural anesthesia improves pancreatic perfusion and decreases the severity of acute pancreatitis
- PMID: 26604652
- PMCID: PMC4649128
- DOI: 10.3748/wjg.v21.i43.12448
Epidural anesthesia improves pancreatic perfusion and decreases the severity of acute pancreatitis
Abstract
Aim: To study the safety of epidural anesthesia (EA), its effect on pancreatic perfusion and the outcome of patients with acute pancreatitis (AP).
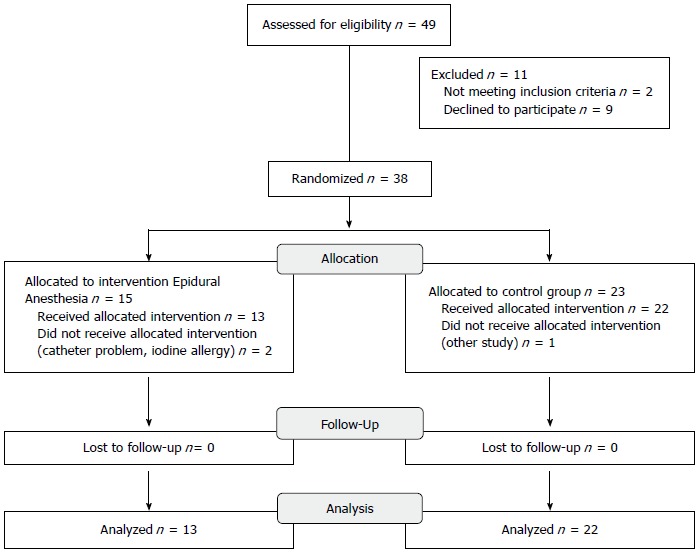
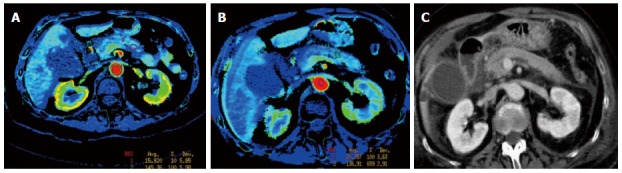
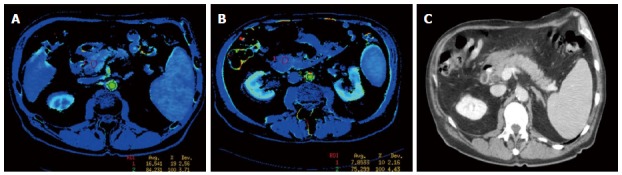
Methods: From 2005 to August 2010, patients with predicted severe AP [Ranson score ≥ 2, C-reactive protein > 100 or necrosis on computed tomography (CT)] were prospectively randomized to either a group receiving EA or a control group treated by patient controlled intravenous analgesia. Pain management was evaluated in the two groups every eight hours using the visual analog pain scale (VAS). Parameters for clinical severity such as length of hospital stay, use of antibiotics, admission to the intensive care unit, radiological/clinical complications and the need for surgical necrosectomy including biochemical data were recorded. A CT scan using a perfusion protocol was performed on admission and at 72 h to evaluate pancreatic blood flow. A significant variation in blood flow was defined as a 20% difference in pancreatic perfusion between admission and 72 h and was measured in the head, body and tail of the pancreas.
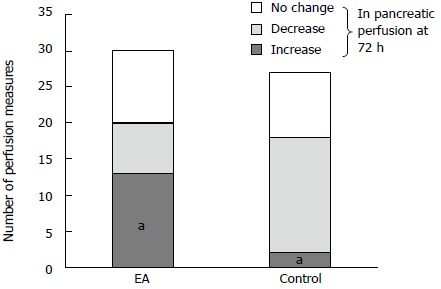
Results: We enrolled 35 patients. Thirteen were randomized to the EA group and 22 to the control group. There were no differences in demographic characteristics between the two groups. The Balthazar radiological severity score on admission was higher in the EA group than in the control group (mean score 4.15 ± 2.54 vs 3.38 ± 1.75, respectively, P = 0.347) and the median Ranson scores were 3.4 and 2.7 respectively (P = NS). The median duration of EA was 5.7 d, and no complications of the epidural procedure were reported. An improvement in perfusion of the pancreas was observed in 13/30 (43%) of measurements in the EA group vs 2/27 (7%) in the control group (P = 0.0025). Necrosectomy was performed in 1/13 patients in the EA group vs 4/22 patients in the control group (P = 0.63). The VAS improved during the first ten days in the EA group compared to the control group (0.2 vs 2.33, P = 0.034 at 10 d). Length of stay and mortality were not statistically different between the 2 groups (26 d vs 30 d, P = 0.65, and 0% for both respectively).
Conclusion: Our study demonstrates that EA increases arterial perfusion of the pancreas and improves the clinical outcome of patients with AP.
Keywords: Computed tomography; Epidural anesthesia; Pancreatic necrosectomy; Pancreatic perfusion; Severe acute pancreatitis.
Figures
References
-
- Yang AL, Vadhavkar S, Singh G, Omary MB. Epidemiology of alcohol-related liver and pancreatic disease in the United States. Arch Intern Med. 2008;168:649–656. - PubMed
-
- Beger HG, Rau B, Isenmann R. Prevention of severe change in acute pancreatitis: prediction and prevention. J Hepatobiliary Pancreat Surg. 2001;8:140–147. - PubMed
-
- Banks PA, Freeman ML. Practice guidelines in acute pancreatitis. Am J Gastroenterol. 2006;101:2379–2400. - PubMed
-
- Schilling MK, Redaelli C, Reber PU, Friess H, Signer C, Stoupis C, Büchler MW. Microcirculation in chronic alcoholic pancreatitis: a laser Doppler flow study. Pancreas. 1999;19:21–25. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
