

Methylphenidate for attention-deficit/hyperactivity disorder in children and adolescents: Cochrane systematic review with meta-analyses and trial sequential analyses of randomised clinical trials
- PMID: 26608309
- PMCID: PMC4659414
- DOI: 10.1136/bmj.h5203
Methylphenidate for attention-deficit/hyperactivity disorder in children and adolescents: Cochrane systematic review with meta-analyses and trial sequential analyses of randomised clinical trials
Abstract
Study question: Is methylphenidate beneficial or harmful for the treatment of attention-deficit/hyperactivity disorder (ADHD) in children and adolescents?
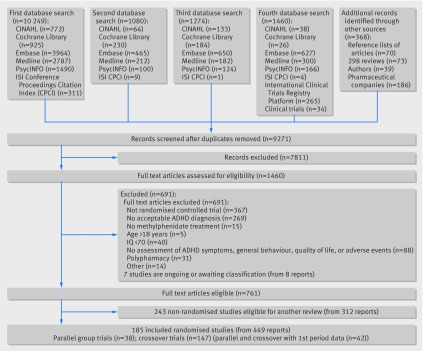
Methods: Electronic databases were searched up to February 2015 for parallel and crossover randomised clinical trials comparing methylphenidate with placebo or no intervention in children and adolescents with ADHD. Meta-analyses and trial sequential analyses (TSA) were conducted. Quality was assessed using GRADE. Teachers, parents, and observers rated ADHD symptoms and general behaviour.
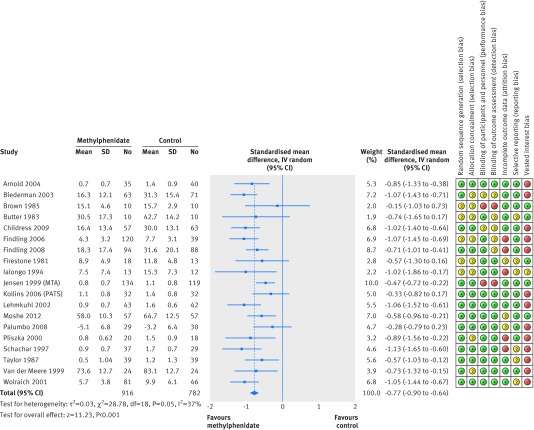
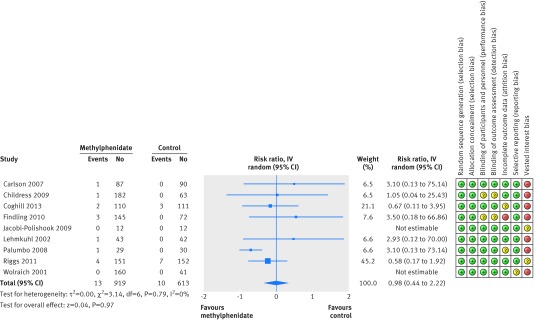
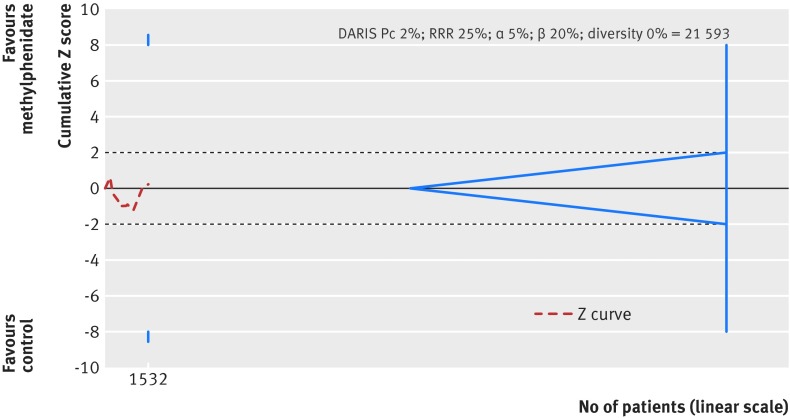
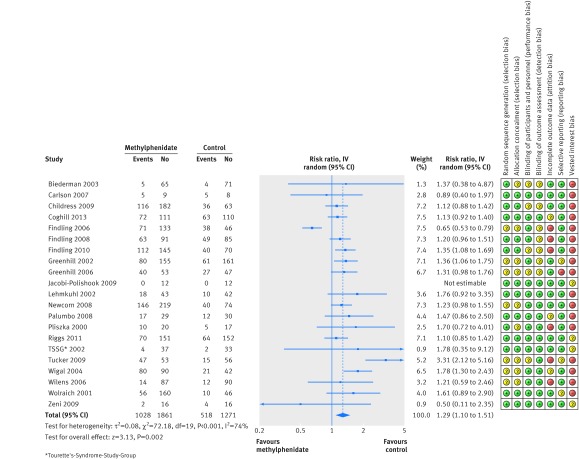
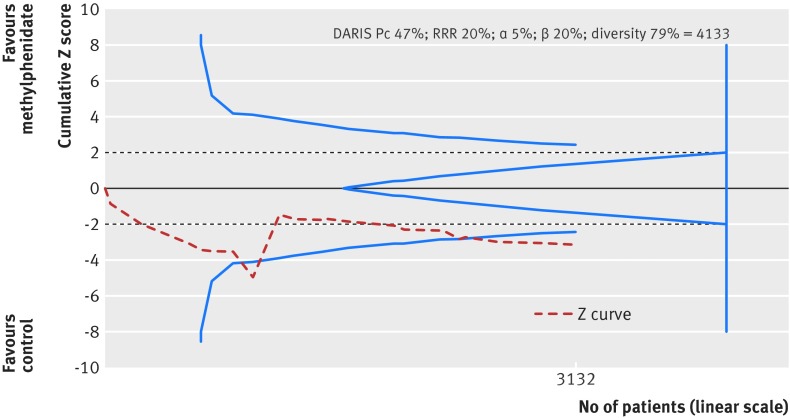
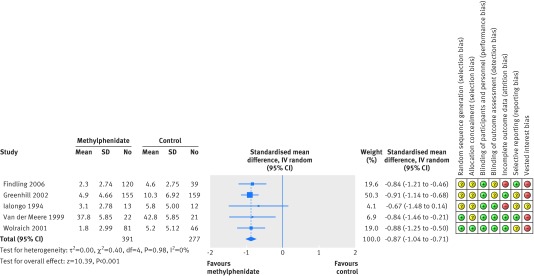
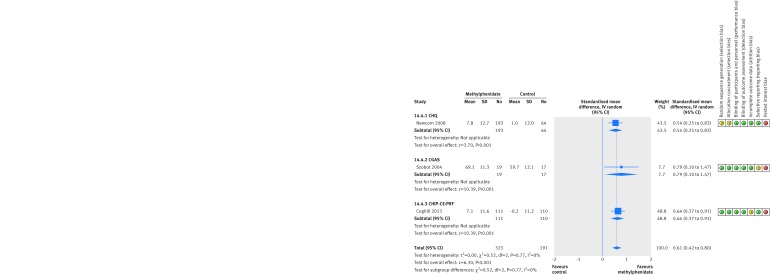
Study answer and limitations: The analyses included 38 parallel group trials (n=5111, median treatment duration 49 days) and 147 crossover trials (n=7134, 14 days). The average age across all studies was 9.7 years. The analysis suggested a beneficial effect of methylphenidate on teacher rated symptoms in 19 parallel group trials (standardised mean difference (SMD) -0.77, n=1698), corresponding to a mean difference of -9.6 points on the ADHD rating scale. There was no evidence that methylphenidate was associated with an increase in serious adverse events (risk ratio 0.98, nine trials, n=1532; TSA adjusted intervention effect RR 0.91). Methylphenidate was associated with an increased risk of non-serious adverse events (1.29, 21 trials, n=3132; TSA adjusted RR 1.29). Teacher rated general behaviour seemed to improve with methylphenidate (SMD -0.87, five trials, n=668) A change of 7 points on the child health questionnaire (CHQ) has been deemed a minimal clinically relevant difference. The change reported in a meta-analysis of three trials corresponds to a mean difference of 8.0 points on the CHQ (range 0-100 points), which suggests that methylphenidate may improve parent reported quality of life (SMD 0.61, three trials, n=514). 96.8% of trials were considered high risk of bias trials according to the Cochrane guidelines. All outcomes were assessed very low quality according to GRADE.
What this study adds: The results suggest that among children and adolescents with a diagnosis of ADHD, methylphenidate may improve teacher reported symptoms of ADHD and general behaviour and parent reported quality of life. However, given the risk of bias in the included studies, and the very low quality of outcomes, the magnitude of the effects is uncertain. Methylphenidate is associated with an increased risk of non-serious but not serious adverse events.
Funding, competing interests, data sharing: Region Zealand Research Foundation and Copenhagen Trial Unit. Competing interests are given in the full paper on bmj.com. Full data are available in the version of this review published in The Cochrane Library.
© Storebø et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure for at
Figures
Comment in
-
Methylphenidate for ADHD.BMJ. 2015 Nov 25;351:h5875. doi: 10.1136/bmj.h5875. BMJ. 2015. PMID: 26608974 No abstract available.
References
-
- Scahill L, Schwab-Stone M. Epidemiology of ADHD in school-age children. Child Adolesc Psychiatr Clin N Am 2000;9:541-55. - PubMed
-
- Polanczyk GV, Salum GA, Sugaya LS, Caye A, Rohde LA. Annual research review: a meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J Child Psychol Psychiatry 2015;56:345-65. - PubMed
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders : DSM-5. APA; 2013.
-
- World Health Organization. The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. WHO; 1992.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials