

Improving detection of familial hypercholesterolaemia in primary care using electronic audit and nurse-led clinics
- PMID: 26608940
- PMCID: PMC4840360
- DOI: 10.1111/jep.12481
Improving detection of familial hypercholesterolaemia in primary care using electronic audit and nurse-led clinics
Abstract
Rationale, aims and objectives: In the UK fewer than 15% of familial hypercholesterolemia (FH) cases are diagnosed, representing a major gap in coronary heart disease prevention. We wished to support primary care doctors within the Medway Clinical Commissioning Group (CCG) to implement NICE guidance (CG71) and consider the possibility of FH in adults who have raised total cholesterol concentrations, thereby improving the detection of people with FH.
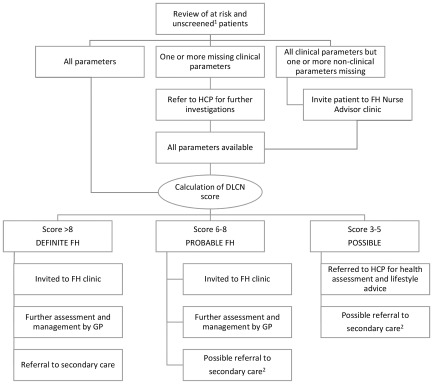
Methods: Utilizing clinical decision support software (Audit+) we developed an FH Audit Tool and implemented a systematic audit of electronic medical records within GP practices, first identifying all patients diagnosed with FH or possible FH and next electronically flagging patients with a recorded total cholesterol of >7.5 mmol L(-1) or LDL-C > 4.9 mmol L(-1) (in adults), for further assessment. After a 2-year period, a nurse-led clinic was introduced to screen more intensely for new FH index cases. We evaluated if these interventions increased the prevalence of FH closer to the expected prevalence from epidemiological studies.
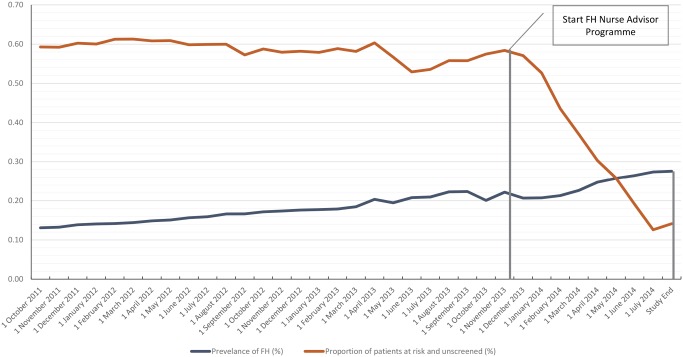
Results: The baseline prevalence of FH within Medway CCG was 0.13% (1 in 750 persons). After 2 years, the recorded prevalence of diagnosed FH increased by 0.09% to 0.22% (1 in 450 persons). The nurse advisor programme ran for 9 months (October 2013-July 2014) and during this time, the recorded prevalence of patients diagnosed with FH increased to 0.28% (1 in 357 persons) and the prevalence of patients 'at risk and unscreened' reduced from 0.58% to 0.14%.
Conclusions: Our study shows that two simple interventions increased the detection of FH. This systematic yet simple electronic case-finding programme with nurse-led review allowed the identification of new index cases, more than doubling the recorded prevalence of detected disease to 1 in 357 (0.28%). This study shows that primary care has an important role in identifying patients with this condition.
Keywords: audit; clinical decision making; clinical guidelines; diagnosis; familial hypercholesterolaemia; prevention.
© 2015 The Authors. Journal of Evaluation in Clinical Practice published by John Wiley & Sons, Ltd.
Figures
References
-
- Marks, D. , Thorogood, M. , Neil, H. A. & Humphries, S. E. (2003) A review on the diagnosis, natural history, and treatment of familial hypercholesterolaemia. Atherosclerosis, 168, 1–14. - PubMed
-
- National Institute for Health and Care Excellence (2008) Clinical guidelines and evidence review for familial hypercholesterolaemia: the identification and management of adults and children with familial hypercholesterolaemia. London: NICE. (Clinical Guideline 71). Available at: www.nice.org.uk/CG71 (last accessed October 2014).
-
- National Institute for Health and Care Excellence (2013) Familial hypercholesterolaemia. London: NICE. (Quality Standards 41). Available at: www.nice.org.uk/QS41 (last accessed August 2015).
-
- Nordestgaard, B. G. , Chapman, M. J. , Humphries, S. E. , et al (2013) Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: guidance for clinicians to prevent coronary heart disease. Consensus Statement of the European Atherosclerosis Society. European Heart Journal, 34, 3478–3490. - PMC - PubMed
-
- Watts, G. F. , Gidding, S. , Wierzbicki, A. S. , et al (2014) Integrated guidance on the care of familial hypercholesterolaemia from the International FH Foundation. International Journal of Cardiology, 171, 309–325. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
