

Ultrasonography of thyroid nodules: a pictorial review
- PMID: 26611469
- PMCID: PMC4729706
- DOI: 10.1007/s13244-015-0446-5
Ultrasonography of thyroid nodules: a pictorial review
Abstract
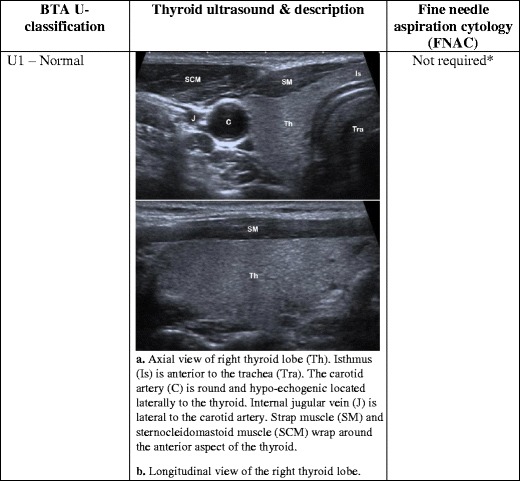
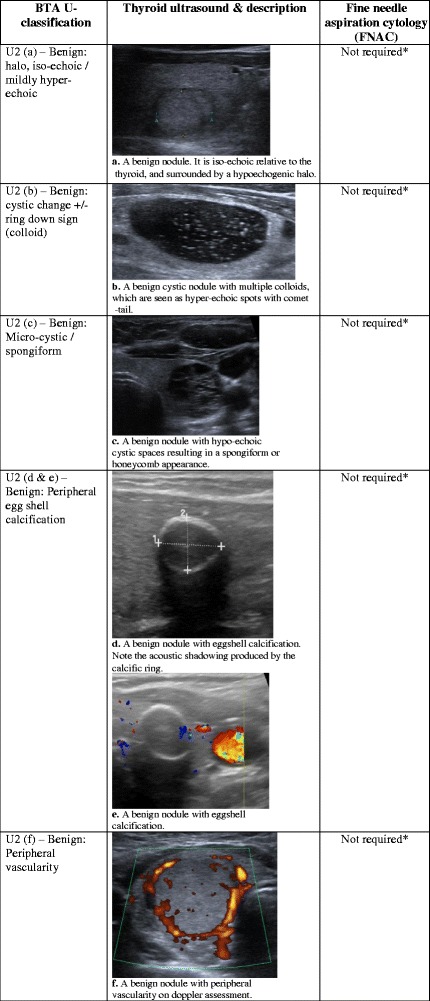
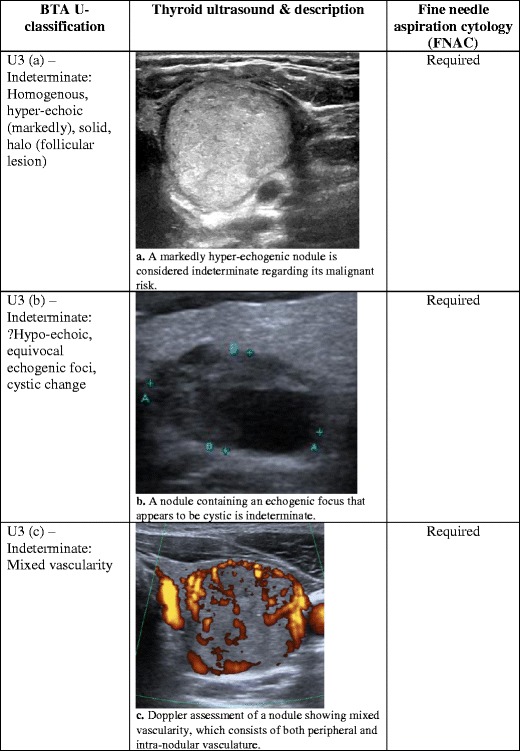
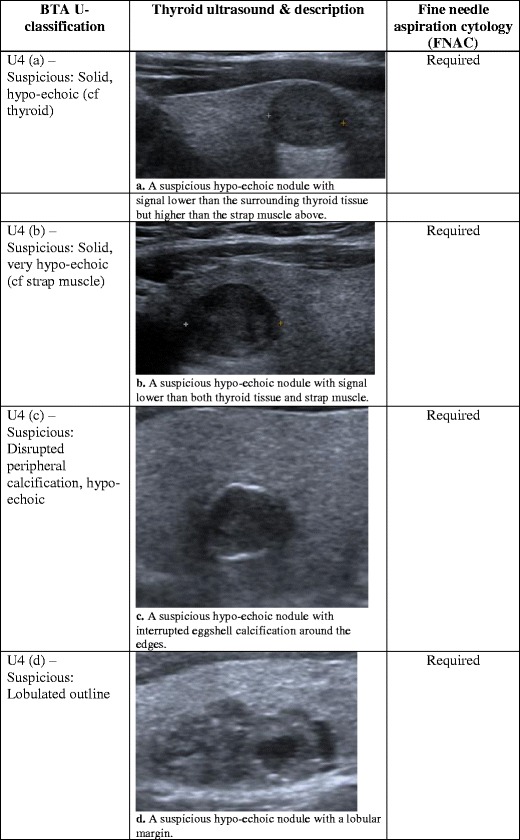
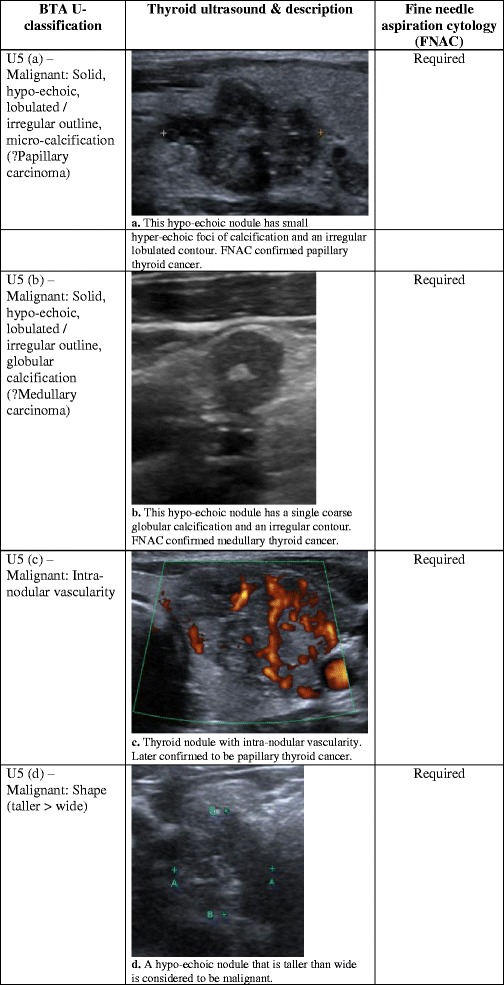
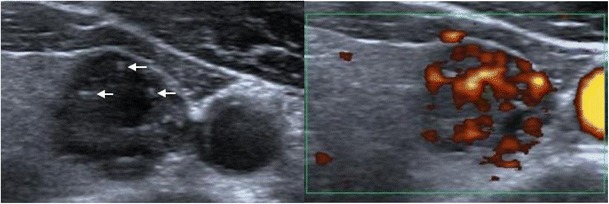
Thyroid nodules are a common occurrence in the general population, and these incidental thyroid nodules are often referred for ultrasound (US) evaluation. US provides a safe and fast method of examination. It is sensitive for the detection of thyroid nodules, and suspicious features can be used to guide further investigation/management decisions. However, given the financial burden on the health service and unnecessary anxiety for patients, it is unrealistic to biopsy every thyroid nodule to confirm diagnosis. The British Thyroid Association (BTA) has recently produced a US classification (U1-U5) of thyroid nodules to facilitate the decision-making process regarding the need to perform fine-needle aspiration cytology (FNAC) for suspicious cases. In this pictorial review, we provide a complete series of sonographic images to illustrate benign and malignant features of thyroid nodules according to the U1-5 classification. Specifically, we highlight morphologic characteristic of the nodule, including its echo signal in relation to its consistency, nodular size, number and contour. Additional diagnostic features such as halo, colloid, calcification and vascular patterns are also discussed in detail. The aim is to assist radiologists and clinicians in recognising sonographic patterns of benign, suspicious and malignant nodules based on U1-5 criteria, and in planning for further investigations.
Main messages: • Ultrasound is sensitive in identifying suspicious features, which require aspiration. • Whether nodules require aspiration should be based on sonographic features and clinical findings. • U1-5 classification of sonographic findings can help determine whether aspiration is necessary.
Keywords: Fine-needle aspiration; Sonographic features; Thyroid cancer; Thyroid nodule; Ultrasound.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources
