

Prenatal interventions for congenital diaphragmatic hernia for improving outcomes
- PMID: 26611822
- PMCID: PMC8947621
- DOI: 10.1002/14651858.CD008925.pub2
Prenatal interventions for congenital diaphragmatic hernia for improving outcomes
Abstract
Background: Congenital diaphragmatic hernia (CDH), is an uncommon but severe condition in which there is a developmental defect in the fetal diaphragm, resulting in liver and bowel migrating to the chest cavity and impairing lung development and function for the neonate. This condition can be diagnosed during pregnancy and as such, is potentially amenable to in-utero prenatal intervention. Neonatal surgical repair is possible, but even with early surgical repair and improving neonatal management, neonatal morbidity and mortality is high. Prenatal interventions described to date have included maternal antenatal corticosteroid administration and fetal tracheal occlusion, with both methods aiming to improve lung growth and maturity. However surgical procedures have potential maternal complications, as the uterus and amniotic sac are breached in order to gain access to the fetus.
Objectives: To compare the effects of prenatal versus postnatal interventions for CDH on perinatal mortality and morbidity, longer-term infant outcomes and maternal morbidity, and to compare the effects of different prenatal interventions with each other.
Search methods: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (31 August 2015) and reference lists of retrieved studies.
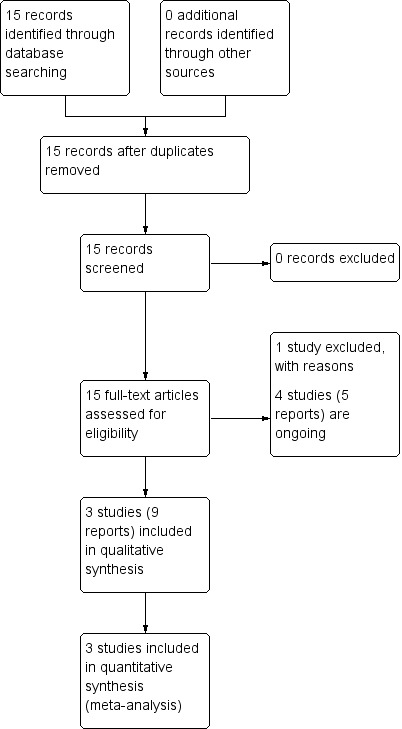
Selection criteria: All published (including those published in abstract form), unpublished, and ongoing randomised controlled trials comparing prenatal and postnatal interventions for fetuses with CDH. Quasi-RCTs were eligible for inclusion but none were identified. Trials using a cross-over design are not eligible for inclusion.
Data collection and analysis: Two review authors evaluated trials for inclusion and methodological quality without consideration of their results according to the stated eligibility criteria and extracted data independently. Data were checked for accuracy.
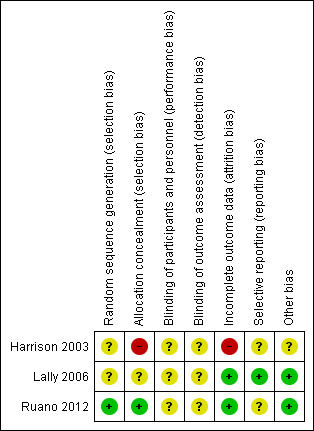
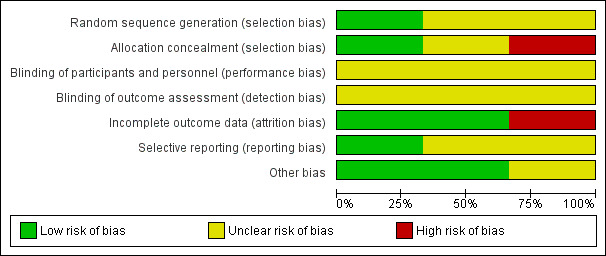
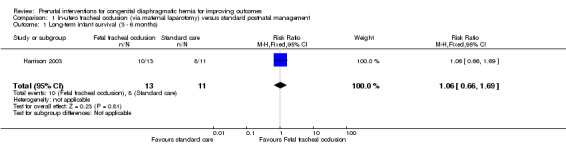
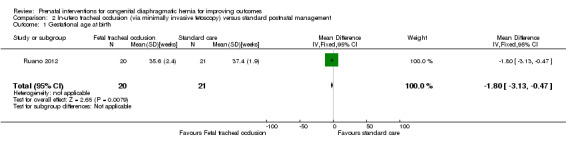
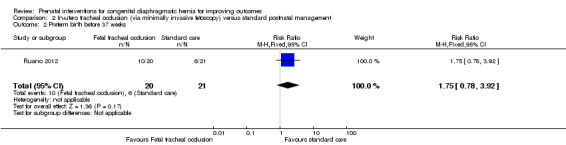
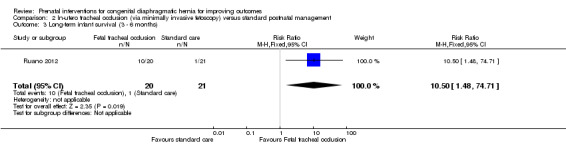
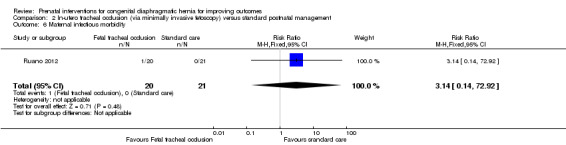
Main results: We identified 11 studies for potential inclusion. Of those, we included three studies involving 97 women. Two additional studies are ongoing.Two trials examined in-utero fetal tracheal occlusion with standard (postnatal) care in fetuses with severe diaphragmatic hernia. Whilst the trials utilised fetal interventions that were similar, there were important differences in how access was gained to the fetus and in the timing and mode of delivery. Therefore, we did not combine these trials in meta-analysis and the results are examined in separate comparisons. One trial examined the effect of antenatal corticosteroids versus placebo. Overall, the methodological quality of the trials was variable and no data were available for a number of this review's secondary outcomes. In-utero fetal occlusion by maternal laparotomy versus standard postnatal management (one trial, 24 women)For the primary infant outcome (perinatal mortality), there were no data suitable for inclusion in the analysis. There was no difference between groups in terms of long-term infant survival (risk ratio (RR) 1.06, 95% confidence interval (CI) 0.66 to 1.69). In-utero fetal occlusion by minimally invasive fetoscopy versus standard postnatal management (one trial, 41 women)The primary infant outcome (perinatal mortality) was not reported. Minimally invasive fetoscopy was associated with a small reduction in the mean gestational age at birth (mean difference (MD) -1.80 weeks, 95% CI -3.13 to -0.47), but there was no clear difference in the risk of preterm birth before 37 weeks (RR 1.75, 95% CI 0.78 to 3.92). Long-term infant survival (three to six months) (RR 10.50, 95% CI 1.48 to 74.71) was increased with the intervention when compared with standard management, and there was a corresponding reduction in pulmonary hypertension (RR 0.58, 95% CI 0.36 to 0.93) associated with the intervention. There was no difference between groups in terms of preterm ruptured membranes (< 37 weeks) (RR 1.47, 95% CI 0.56 to 3.88) or maternal infectious morbidity (RR 3.14, 95% CI 0.14 to 72.92), and there were no maternal blood transfusions. Antenatal corticosteroids versus placebo (one trial, 32 women)We also included one trial (involving 32 women) examining the effect of antenatal corticosteroids versus placebo. There was no clear difference in the incidence of perinatal mortality (our primary infant outcome) between the group of women who received antenatal corticosteroids and the placebo control (RR 1.24, 95% CI 0.50 to 3.08). Data (mean only) were reported for two of our secondary outcomes (mechanical ventilation and days of hospital admission) but standard deviations (SDs) were not provided. For the purposes of this review and to permit further analysis we have estimated the SDs based on the reported P values reported in the trial report, although our estimation does assume that the SD is the same in both the intervention and control groups. There were no differences between the antenatal corticosteroid group and the placebo control in terms of days of mechanical ventilation (MD 18.00 days, 95% CI -14.77 to 50.77) or days of hospital admission (MD 17.00 days, 95% CI -13.93 to 47.93) .
Authors' conclusions: There is currently insufficient evidence to recommend in-utero intervention for fetuses with CDH as a part of routine clinical practice. We identified three small studies, with only one study adequately reporting on the primary outcome of this review - perinatal mortality, and there were few data pertaining to many of this review's secondary outcomes.WIth regard to the administration of antenatal corticosteroids, there remains a gap in current research, and a large multicentre trial with adequate statistical power should be undertaken to answer this unresolved question. More studies are needed to further examine the effect of in-utero fetal tracheal occlusion on important neonatal outcomes and long-term infant survival and health. Long-term follow-up is of particular importance, and should include morbidity and mortality measures. Further studies should examine the benefits of an in-utero intervention on subgroups with moderate and severe congenital diaphragmatic hernia. Indeed, there are three ongoing studies, being conducted by European, North and South American fetal medicine centres, which will contribute to this gap. Ongoing research and any implementation into clinical practice should include standardisation of the procedure, inclusion criteria and long-term childhood follow-up.
Conflict of interest statement
None known.
Figures




Update of
References
References to studies included in this review
Harrison 2003 {published data only}
-
- Albanese C, Farrell J. Congenital diaphragmatic hernia ‐ a randomized clinical trial. Frontiers in Fetal Health 2000;2(6):1‐4.
-
- Cortes RA, Keller RL, Townsend T, Harrison MR, Farmer DL, Lee H, et al. Survival of severe congenital diaphragmatic hernia has morbid consequences. Journal of Pediatric Surgery 2005;40(1):36‐45. - PubMed
-
- Harrison MR, Keller RL, Hawgood SB, Kitterman JA, Sandberg PL, Farmer DL, et al. A randomized trial of fetal endoscopic tracheal occlusion for severe fetal congenital diaphragmatic hernia. New England Journal of Medicine 2003;349:1916‐24. - PubMed
-
- Keller RL, Hawgood S, Neuhaus JM, Farmer DL, Lee H, Albanese CT, et al. Infant pulmonary function in a randomized trial of fetal tracheal occlusion for severe congenital diaphragmatic hernia. Pediatric Research 2004;56(5):818‐25. - PubMed
Lally 2006 {published data only}
-
- Lally KP, Bagolan P, Hosie S, Lally PA, Stewart M, Cotten CM, et al. Corticosteroids for fetuses with congenital diaphragmatic hernia: can we show benefit?. Journal of Pediatric Surgery 2006;41(4):668‐74. - PubMed
Ruano 2012 {published data only}
-
- Ruano R. Tracheal occlusion guided by percutaneous fetoscopy in fetuses with severe isolated congenital diaphragmatic hernia. http://clinicaltrials.gov/ct2/show/record/NCT01302977 (accessed 16 December 2011) 2011.
-
- Ruano R, Duarte S, Silva M, Tannuri U, Zugaib M. Fetal endoscopic tracheal occlusion in severe congenital diaphragmatic hernia using 1.0 mm fetoscope ‐ preliminary results of a randomized study. International Journal of Gynecology & Obstetrics 2009;107(Suppl 2):S325.
-
- Ruano R, Yoshisaki CT, Silva MM, Ceccon ME, Grasi MS, Tannuri U, et al. A randomized controlled trial of fetal endoscopic tracheal occlusion versus postnatal management of severe isolated congenital diaphragmatic hernia. Ultrasound in Obstetrics & Gynecology 2012;39(1):20‐7. - PubMed
-
- Ruano S, Duarte SA, Silva MM, Tannuri, Zugaib M. Fetal endoscopic tracheal occlusion in severe congenital diaphragmatic hernia using 1.0 mm fetoscope ‐ a randomised study. Ultrasound in Obstetrics & Gynecology 2009;34:132.
References to studies excluded from this review
Belfort 2011 {published data only}
-
- Belfort M. The effectiveness of fetal endotracheal occlusion (feto) in the management of severe congenital diaphragmatic hernia. http://clinicaltrials.gov/ct2/show/NCT00881660 (accessed 1 December 2011) 2011.
References to ongoing studies
Deprest 2009b {published data only}
-
- Dekoninck P, Gratacos E, Mieghem T, Richter J, Lewi P, Ancel AM, et al. Results of fetal endoscopic tracheal occlusion for congenital diaphragmatic hernia and the set up of the randomized controlled TOTAL trial. Early Human Development 2011;87(9):619‐24. - PubMed
-
- Deprest J. Randomized control trial of fetoscopic endoluminal tracheal occlusion with a balloon versus expectant management during pregnancy in fetuses with left sided congenital diaphragmatic hernia and moderate pulmonary hypoplasia (TOTAL). http://clinicaltrials.gov/ct2/show/NCT00763737 (accessed 4 January 2009).
-
- Deprest J, Nicolaides K, Tibboel D, Ville Y, Reiss I, Gratacos E. Total randomized controlled trial for moderate pulmonary hypoplasia due to congenital diaphragmatic hernia (CDH). Ultrasound in Obstetrics & Gynecology 2009;34(Suppl 1):91.
Kohl 2006 {published data only}
-
- Kohl T. Randomized clinical trial in order to assess the effect of fetoscopic tracheal balloon occlusion on the postnatal disease course in neonates with left congenital diaphragmatic hernia. http://clinicaltrials.gov/ct2/show/record/NCT00373438 (accessed 19 December 2011).
Ruano 2013 {published data only}
-
- Ruano R. "Early" versus "standard" fetal endoscopic tracheal occlusion for severe congenital diaphragmatic hernia ‐ a randomized controlled trial. http://clinicaltrials.gov/show/NCT01731509 (accessed 24 October 2013).
Additional references
AIHW 2004
-
- AIHW National Perinatal Statistics Unit. Australia's Babies: Their Health and Wellbeing. Bulletin no. 21. AIHW cat. no. AUS 54. Camberra: AIHW NPSU, 2004.
Chiu 2006
-
- Chiu PP, Sauer C, Mihailovic A, Adatia I, Bohn D, Coates AL, et al. The price of success in the management of congenital diaphragmatic hernia: is improved survival accompanied by an increase in long‐term morbidity?. Journal of Pediatric Surgery 2006;41(5):888‐92. - PubMed
Chiu 2008
-
- Chiu P, Hedrick HL. Postnatal management and long‐term outcome for survivors with congenital diaphragmatic hernia. Prenatal Diagnosis 2008;28(7):592‐603. - PubMed
Colvin 2005
-
- Colvin J, Bower C, Dickinson J, Sokol J. Outcomes of congenital diaphragmatic hernia: a population‐based study in Western Australia. Pediatrics 2005;116(3):356‐63. - PubMed
Cundy 2013
-
- Cundy TP, Gardener GJ, Andersen CC, Kirby CP, McBride CA, Teague WJ. Fetoscopic endoluminal tracheal occlusion (FETO) for congenital diaphragmatic hernia in Australia and New Zealand: are we willing, able, both or neither?. Journal of Paediatrics and Child Health 2013;50(3):226‐33. - PubMed
Deprest 2004
-
- Deprest J, Gratacos E, Nicolaides KH, FETO Task Group. Fetoscopic tracheal occlusion (FETO) for severe congenital diaphragmatic hernia: evolution of a technique and preliminary results. Ultrasound in Obstetrics and Gynecology 2004;24(2):121‐6. - PubMed
Deprest 2009a
-
- Deprest JA, Gratacos E, Nicolaides K, Done E, Mieghem T, Gucciardo L, et al. Changing perspectives on the perinatal management of isolated congenital diaphragmatic hernia in Europe. Clinics in Perinatology 2009;36:329‐47. - PubMed
DiFiore 1994
-
- DiFiore JW, Fauza DO, Slavin R, Peters CA, Fackler JC, Wilson JM. Experimental fetal tracheal ligation reverses the structural and physiological effects of pulmonary hypoplasia in congenital diaphragmatic hernia. Journal of Pediatric Surgery 1994;29(2):248‐56. - PubMed
Done 2008
-
- Done E, Gucciardo L, Mieghem T, Jani J, Cannie M, Schoubroeck D, et al. Prenatal diagnosis, prediction of outcome and in utero therapy of isolated congenital diaphragmatic hernia. Prenatal Diagnosis 2008;28(7):581‐91. - PubMed
George 1987
-
- George DK, Cooney TP, Chiu BK, Thurlbeck WM. Hypoplasia and immaturity of the terminal lung unit (acinus) in congenital diaphragmatic hernia. American Review of Respiratory Disease 1987;136(4):947‐50. - PubMed
Gross 1946
-
- Gross RE. Congenital hernia of the diaphragm. American Journal of Diseases of Children 1946;71:579‐92. - PubMed
Harrison 1997
-
- Harrison MR, Adzick NS, Bullard KM, Farrell JA, Howell LS, Rosen MA, et al. Correction of congenital diaphragmatic hernia in utero. VII. A prospective trial. Journal of Pediatric Surgery 1997;32(11):1637‐42. - PubMed
Higgins 2011
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Laudy 2003
-
- Laudy JA, Gucht M, Dooren MF, Wladimiroff JW, Tibboel D. Congenital diaphragmatic hernia: an evaluation of the prognostic value of the lung‐to‐head ratio and other prenatal parameters. Prenatal Diagnosis 2003;23(8):634‐9. - PubMed
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous