

Upper Airway Collapsibility (Pcrit) and Pharyngeal Dilator Muscle Activity are Sleep Stage Dependent
- PMID: 26612386
- PMCID: PMC4763361
- DOI: 10.5665/sleep.5516
Upper Airway Collapsibility (Pcrit) and Pharyngeal Dilator Muscle Activity are Sleep Stage Dependent
Abstract
Study objectives: An anatomically narrow/highly collapsible upper airway is the main cause of obstructive sleep apnea (OSA). Upper airway muscle activity contributes to airway patency and, like apnea severity, can be sleep stage dependent. Conversely, existing data derived from a small number of participants suggest that upper airway collapsibility, measured by the passive pharyngeal critical closing pressure (Pcrit) technique, is not sleep stage dependent. This study aimed to determine the effect of sleep stage on Pcrit and upper airway muscle activity in a larger cohort than previously tested.
Methods: Pcrit and/or muscle data were obtained from 72 adults aged 20-64 y with and without OSA.Pcrit was determined via transient reductions in continuous positive airway pressure (CPAP) during N2, slow wave sleep (SWS) and rapid eye movement (REM) sleep. Genioglossus and tensor palatini muscle activities were measured: (1) awake with and without CPAP, (2) during stable sleep on CPAP, and (3) in response to the CPAP reductions used to quantify Pcrit.
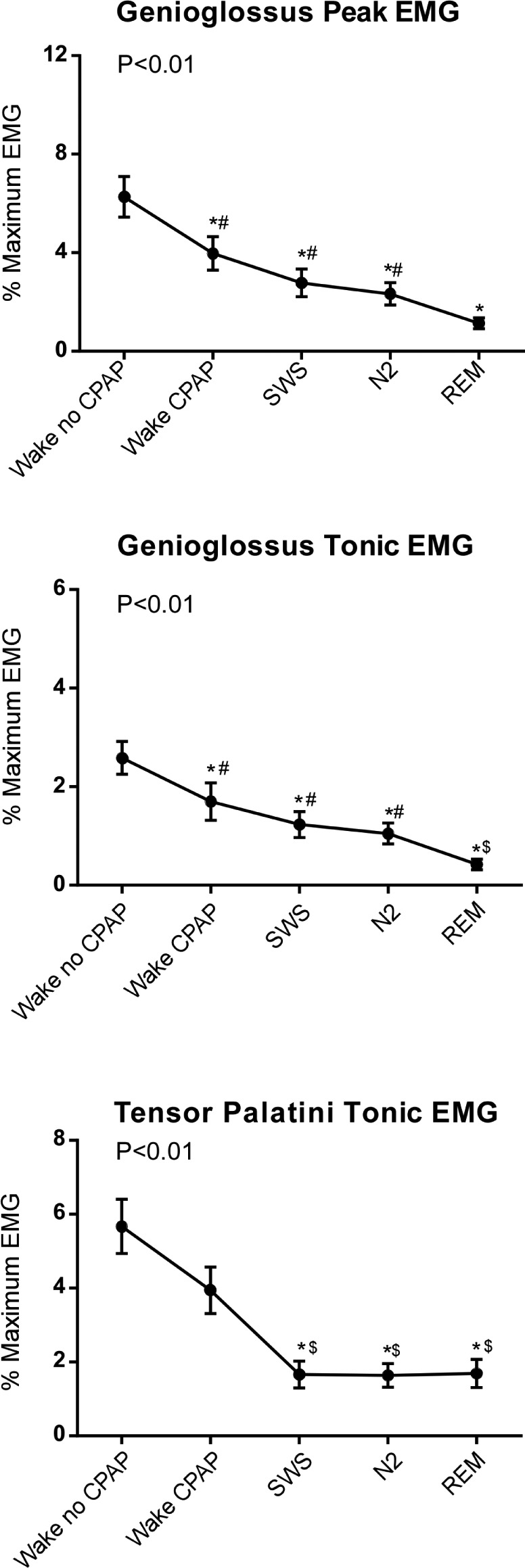
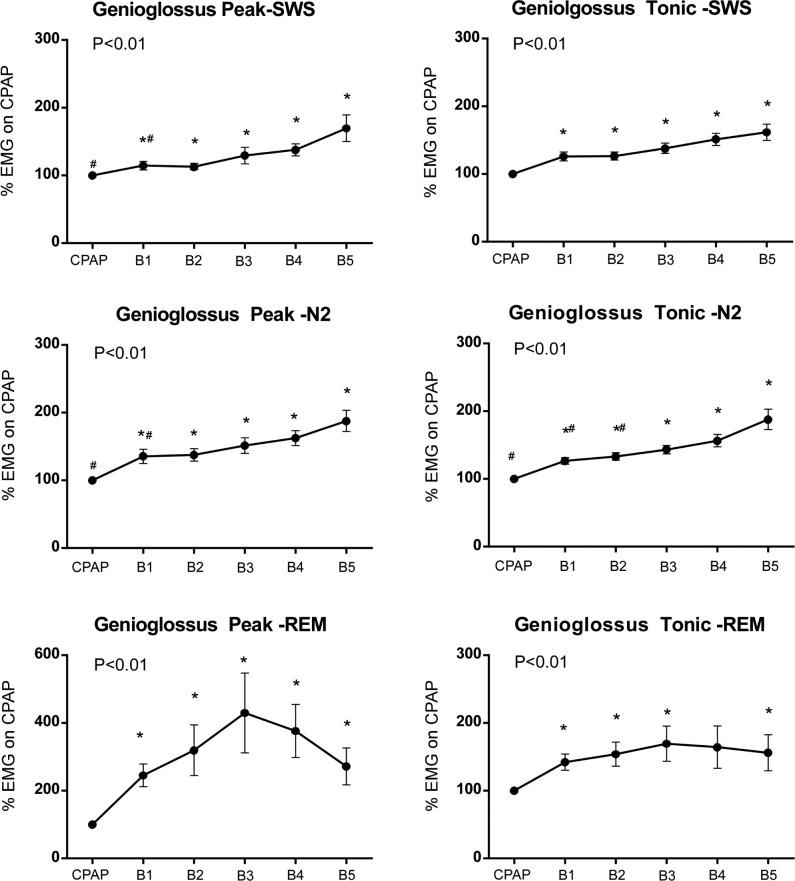
Results: Pcrit was 4.9 ± 1.4 cmH2O higher (more collapsible) during REM versus SWS (P = 0.012), 2.3 ± 0.6 cmH2O higher during REM versus N2 (P < 0.001), and 1.6 ± 0.7 cmH2O higher in N2 versus SWS (P = 0.048). Muscle activity decreased from wakefulness to sleep and from SWS to N2 to REM sleep for genioglossus but not for tensor palatini. Pharyngeal muscle activity increased by ∼50% by breath 5 following CPAP reductions.
Conclusions: Upper airway collapsibility measured via the Pcrit technique and genioglossus muscle activity vary with sleep stage. These findings should be taken into account when performing and interpreting "passive" Pcrit measurements.
Keywords: airway anatomy; electromyography; sleep disordered breathing; upper airway physiology.
© 2016 Associated Professional Sleep Societies, LLC.
Figures




References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
