

Association of Coffee Consumption With Overall and Cause-Specific Mortality in a Large US Prospective Cohort Study
- PMID: 26614599
- PMCID: PMC5875735
- DOI: 10.1093/aje/kwv146
Association of Coffee Consumption With Overall and Cause-Specific Mortality in a Large US Prospective Cohort Study
Abstract
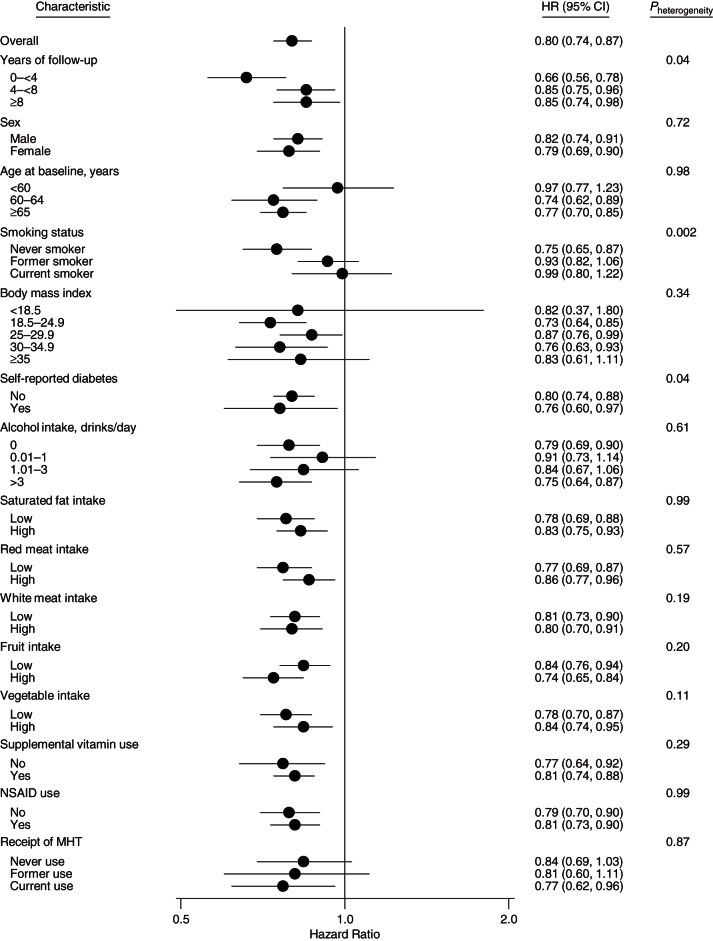
Concerns about high caffeine intake and coffee as a vehicle for added fat and sugar have raised questions about the net impact of coffee on health. Although inverse associations have been observed for overall mortality, data for cause-specific mortality are sparse. Additionally, few studies have considered exclusively decaffeinated coffee intake or use of coffee additives. Coffee intake was assessed at baseline by self-report in the Prostate, Lung, Colorectal and Ovarian Cancer Screening Trial. Hazard ratios were estimated using Cox proportional hazards models. Among 90,317 US adults without cancer at study baseline (1998-2001) or history of cardiovascular disease at study enrollment (1993-2001), 8,718 deaths occurred during 805,644 person-years of follow-up from 1998 through 2009. Following adjustment for smoking and other potential confounders, coffee drinkers, as compared with nondrinkers, had lower hazard ratios for overall mortality (<1 cup/day: hazard ratio (HR) = 0.99 (95% confidence interval (CI): 0.92, 1.07); 1 cup/day: HR = 0.94 (95% CI: 0.87, 1.02); 2-3 cups/day: HR = 0.82 (95% CI: 0.77, 0.88); 4-5 cups/day: HR = 0.79 (95% CI: 0.72, 0.86); ≥6 cups/day: HR = 0.84 (95% CI: 0.75, 0.95)). Similar findings were observed for decaffeinated coffee and coffee additives. Inverse associations were observed for deaths from heart disease, chronic respiratory diseases, diabetes, pneumonia and influenza, and intentional self-harm, but not cancer. Coffee may reduce mortality risk by favorably affecting inflammation, lung function, insulin sensitivity, and depression.
Keywords: additives; caffeine; cause-specific mortality; coffee; mortality.
Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health 2015. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Figures

References
-
- National Coffee Association. National Coffee Drinking Trends. New York, NY: National Coffee Association; 2014.
-
- Coffee drinking and acute myocardial infarction: report from the Boston Collaborative Drug Surveillance Program. Lancet. 1972;27790:1278–1281. - PubMed
-
- Jick H, Miettinen OS, Neff RK et al. Coffee and myocardial infarction. N Engl J Med. 1973;2892:63–67. - PubMed
-
- Wu JN, Ho SC, Zhou C et al. Coffee consumption and risk of coronary heart diseases: a meta-analysis of 21 prospective cohort studies. Int J Cardiol. 2009;1373:216–225. - PubMed
-
- Huxley R, Lee CM, Barzi F et al. Coffee, decaffeinated coffee, and tea consumption in relation to incident type 2 diabetes mellitus: a systematic review with meta-analysis. Arch Intern Med. 2009;16922:2053–2063. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
