

A randomized, placebo-controlled trial of late Na current inhibition (ranolazine) in coronary microvascular dysfunction (CMD): impact on angina and myocardial perfusion reserve
- PMID: 26614823
- PMCID: PMC4872284
- DOI: 10.1093/eurheartj/ehv647
A randomized, placebo-controlled trial of late Na current inhibition (ranolazine) in coronary microvascular dysfunction (CMD): impact on angina and myocardial perfusion reserve
Abstract
Aims: The mechanistic basis of the symptoms and signs of myocardial ischaemia in patients without obstructive coronary artery disease (CAD) and evidence of coronary microvascular dysfunction (CMD) is unclear. The aim of this study was to mechanistically test short-term late sodium current inhibition (ranolazine) in such subjects on angina, myocardial perfusion reserve index, and diastolic filling.
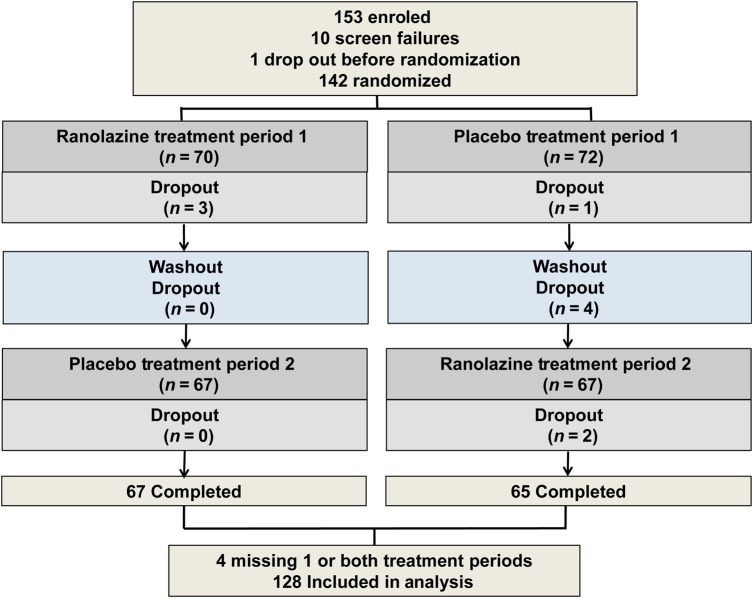
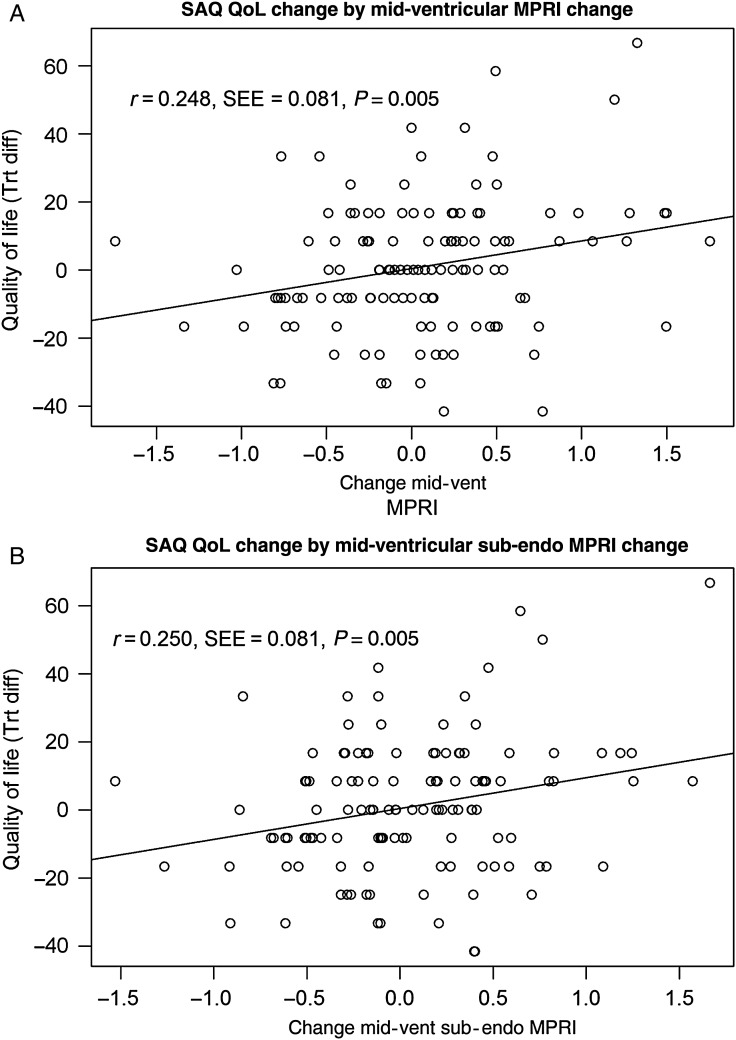
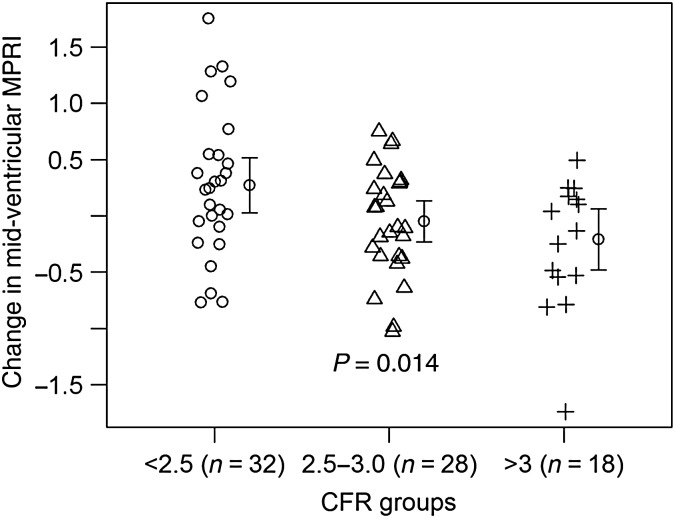
Materials and results: Randomized, double-blind, placebo-controlled, crossover, mechanistic trial in subjects with evidence of CMD [invasive coronary reactivity testing or non-invasive cardiac magnetic resonance imaging myocardial perfusion reserve index (MPRI)]. Short-term oral ranolazine 500-1000 mg twice daily for 2 weeks vs. placebo. Angina measured by Seattle Angina Questionnaire (SAQ) and SAQ-7 (co-primaries), diary angina (secondary), stress MPRI, diastolic filling, quality of life (QoL). Of 128 (96% women) subjects, no treatment differences in the outcomes were observed. Peak heart rate was lower during pharmacological stress during ranolazine (-3.55 b.p.m., P < 0.001). The change in SAQ-7 directly correlated with the change in MPRI (correlation 0.25, P = 0.005). The change in MPRI predicted the change in SAQ QoL, adjusted for body mass index (BMI), prior myocardial infarction, and site (P = 0.0032). Low coronary flow reserve (CFR <2.5) subjects improved MPRI (P < 0.0137), SAQ angina frequency (P = 0.027), and SAQ-7 (P = 0.041).
Conclusions: In this mechanistic trial among symptomatic subjects, no obstructive CAD, short-term late sodium current inhibition was not generally effective for SAQ angina. Angina and myocardial perfusion reserve changes were related, supporting the notion that strategies to improve ischaemia should be tested in these subjects.
Trial registration: clinicaltrials.gov Identifier: NCT01342029.
Keywords: Angina; Coronary microvascular dysfunction.
© The Author 2015. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Treatment of microvascular angina: the need for precision medicine.Eur Heart J. 2016 May 14;37(19):1514-6. doi: 10.1093/eurheartj/ehw021. Epub 2016 Feb 18. Eur Heart J. 2016. PMID: 26896247 No abstract available.
References
-
- Jespersen L, Abildstrom SZ, Hvelplund A, Galatius S, Madsen JK, Pedersen F, Hojberg S, Prescott E. Symptoms of angina pectoris increase the probability of disability pension and premature exit from the workforce even in the absence of obstructive coronary artery disease. Eur Heart J 2013;34:3294–3303. - PubMed
-
- Shaw LJ, Merz CN, Pepine CJ, Reis SE, Bittner V, Kip KE, Kelsey SF, Olson M, Johnson BD, Mankad S, Sharaf BL, Rogers WJ, Pohost GM, Sopko G, Women's Ischemia Syndrome Evaluation I. The economic burden of angina in women with suspected ischemic heart disease: results from the National Institutes of Health—National Heart, Lung, and Blood Institute—sponsored Women's Ischemia Syndrome Evaluation. Circulation 2006;114:894–904. - PubMed
-
- Johnson BD, Shaw LJ, Buchthal SD, Bairey Merz CN, Kim HW, Scott KN, Doyle M, Olson MB, Pepine CJ, den Hollander J, Sharaf B, Rogers WJ, Mankad S, Forder JR, Kelsey SF, Pohost GM. Prognosis in women with myocardial ischemia in the absence of obstructive coronary disease: results from the National Institutes of Health-National Heart, Lung, and Blood Institute-Sponsored Women's Ischemia Syndrome Evaluation (WISE). Circulation 2004;109:2993–2999. - PubMed
-
- Pepine CJ. Ischemic heart disease in women. J Am Coll Cardiol 2006;47(3 Suppl):S1–S3. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
