

Review
doi: 10.1016/j.cden.2015.08.004.
Epub 2015 Oct 21.
Temporomandibular Joint Disorders and Orofacial Pain
Affiliations
- PMID: 26614951
- PMCID: PMC6762033
- DOI: 10.1016/j.cden.2015.08.004
Item in Clipboard
Review
Temporomandibular Joint Disorders and Orofacial Pain
Dent Clin North Am.
2016 Jan.
Abstract
Temporomandibular disorders (TMD) affect 5% to 12% of the United States population. This article discusses common conditions related to temporomandibular joints, including disc displacements, inflammatory disturbances, loose joint bodies, traumatic disturbances, and developmental conditions. Also addressed are the appropriate imaging modalities and diagnostic criteria for TMD.
Keywords: Condylar fracture; Condylar hyperplasia and hypoplasia; DC/TMD; Degenerative joint disease; Diagnostic criteria; Orofacial pain; Synovial chondromatosis; TMJ.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
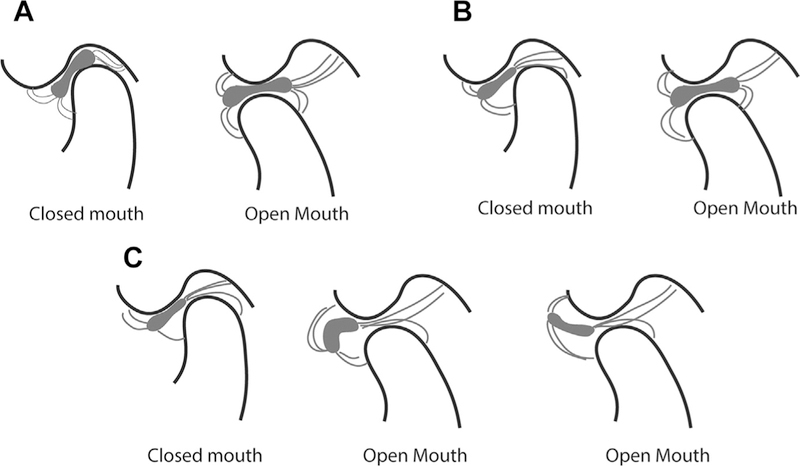
Relationship between bone and articular disc of the temporomandibular joint. (A) Normal disc location in closed- and open-mouth position. In the closed-mouth position, the posterior band of the articular disc is located between 11:30 and 12:30 of a clock face. The central narrow zone of the disc is in contact with the condylar surface and the articular fossa. In the open-mouth position, the central narrow zone of the disc remains in contact with the condylar head and the articular eminence. (B) Disc displacement with reduction. In the closed-mouth position, the posterior band of the articular disc is displaced anterior to 11:30. The central narrow zone of the disc is not in contact with the condyle or the articular fossa. In the open-mouth position, the central narrow zone of the disc is in contact with the condylar head and articular eminence. (C) Disc displacement without reduction. In the closed-mouth position, the posterior band of the articular disc is displaced anterior to 11:30. The central narrow zone of the disc is not in contact with the condyle or the articular fossa. In the open-mouth position, the disc is anteriorly displaced, and may assume a normal biconcave shape or become deformed.
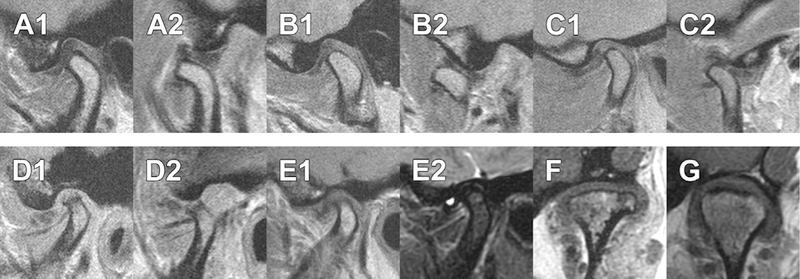
MRI of the temporomandibular joints. A1 and A2 are from the same patient, in closed (A1) and open (A2) mouth position, showing normal disc relationship with the condylar head and articular fossa/eminence. B1 and B2 are from the same patient, in closed (B1) and open (B2) mouth position, showing anteriorly displaced intermediate zone of the disc (B1) and normal disc relationship with condylar head and articular eminence (B2). C1 and C2 are from the same patient, in closed (C1) and open (C2) mouth position, showing disc displacement with reduction. D1 and D2 are from the same patient, in closed (D1) and open (D2) mouth position, showing disc displacement without reduction. E1 and E2 are from the same patient in closed-mouth position. E2, which is a T2-weighted image, shows presence of effusion as a region of bright intensity. (F, G) Axially corrected coronal views from different patients, of (F) normal disc position and (G) laterally displaced disc. All images are proton density except E2.
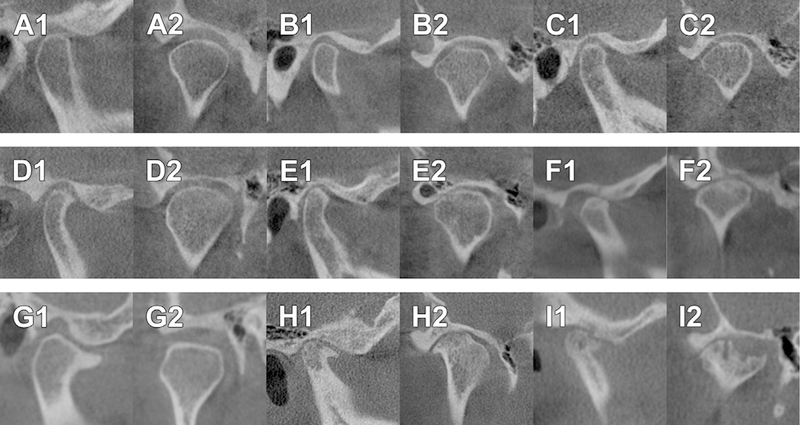
CBCT findings of normal and different representations of degenerative joint disease. A1 and A2 are from the same patient, in corrected sagittal (A1) and corrected coronal (A2) orientations, showing a normal temporomandibular joint, which has smooth, rounded, and well-defined cortical margin of the condyle and the fossa. B1 and B2 are from the same patient, in corrected sagittal (B1) and corrected coronal (B2) orientations, showing flattening of the anterior and lateral slopes of the condylar head, indicating remodeling of the joint. C1 and C2 are from the same patient, in corrected sagittal (C1) and corrected coronal (C2) orientations, showing localized subcortical sclerosis of the condylar head, which indicates remodeling of the joint. The middle panel shows examples of grade 1 DJD. D1 and D2 are from the same patient, in corrected sagittal (D1) and corrected coronal (D2) orientations, showing an osteophyte at the anterior aspect of the condyle. E1 and E2 are from the same patient, in corrected sagittal (E1) and corrected coronal (E2) orientations, showing flattening and subcortical sclerosis of the anterior slope (E1) and localized erosion of the condyle (E2). F1 and F2 are from the same patient, in corrected sagittal (F1) and corrected coronal (F2) orientations, show the presence of a single subcortical pseudocyst. The lower panel shows examples of grade 2 DJD. G1 and G2 are from the same patient, in corrected sagittal (G1) and corrected coronal (G2) orientations, showing an anterior osteophyte larger than 2 mm (G1) and flattening of the superior and lateral slopes of the condyle (G2). H1 and H2 are from the same patient, in corrected sagittal (H1) and corrected coronal (H2) orientations, showing the presence of osteophytes and multiple subcortical pseudocysts. I1 and 12 are from the same patient, in corrected sagittal (I1) and corrected coronal (I2) orientations, showing the presence of osteophytes and multiple areas of erosion, one of which is wider than 2 mm.
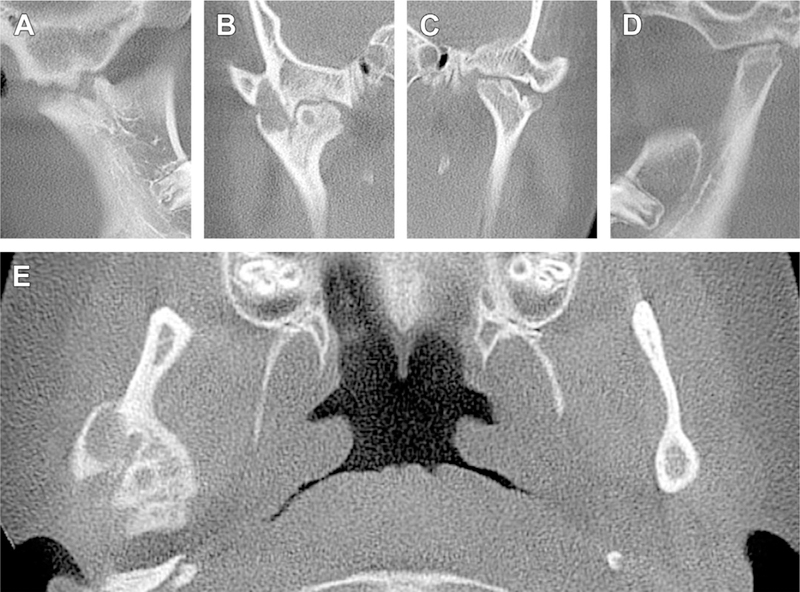
Cone-beam computed tomography of a patient with bilateral involvement with rheumatoid arthritis. (A) Corrected sagittal view of the right joint. Superior margin of the condylar head is irregular. (B) Axially corrected coronal view of the right joint, which shows interdigitation of bony projections that lead to ankylosis of the joint. A subcortical pseudocyst is present in the condylar head. (C, D) Sagittal and coronal sections of the left joint. Superior margin of the left condylar head is irregularly flat and has prominent notching. The articular fossa is also flat. (E) Axial section of the same patient at the level of the right condylar head. Note the excessive enlargement of the right condylar head with subcortical pseudocysts and irregular margins.
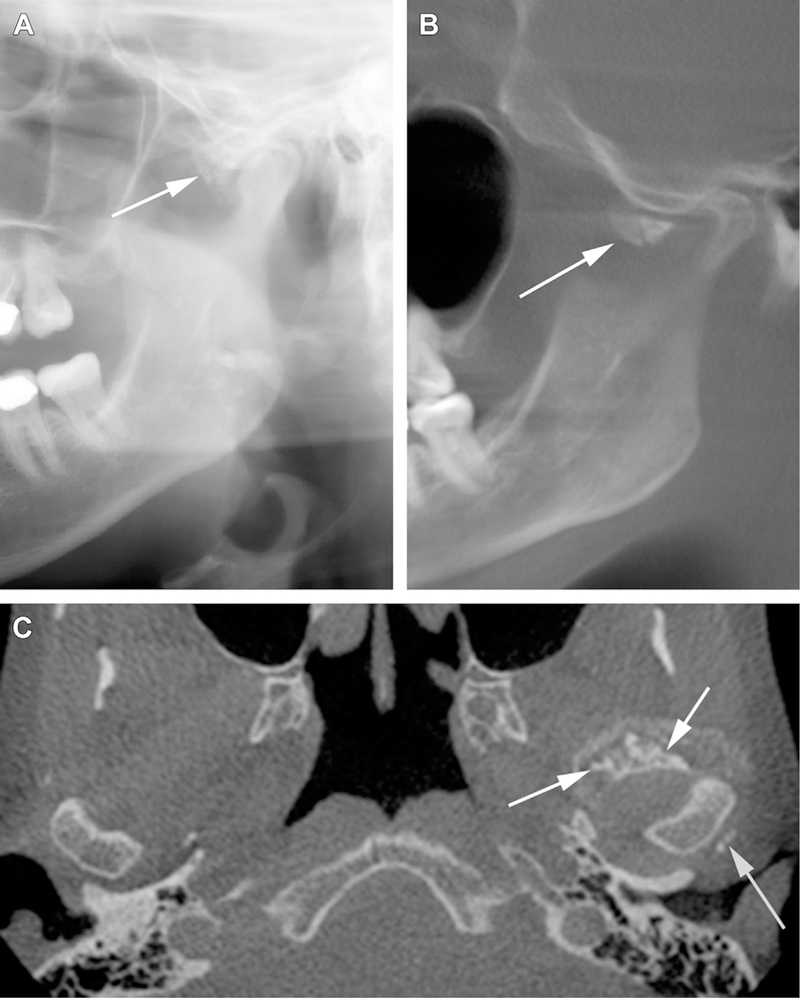
Synovial chondromatosis of the left temporomandibular joint. (A) Sectional panoramic radiograph shows synovial chondromatosis (arrow) associated with the left temporomandibular joint. (B) Section of a reconstructed panoramic view of a CBCT of the same patient, showing presence of synovial chondromatosis (arrow) at the anterior aspect of the left condylar head. (C) Axial view at the level of the TMJs of the left TMJ. Synovial chondromatosis (arrows) is present at the anterior and posterior margins of the condylar head.

Fracture of the condylar heads. (A) Sectional panoramic radiograph of a fractured condylar head superimposed over the neck of the condyle. The displaced fractured fragment is either on the lateral or medial aspect of the neck. (B) Open-mouth Towne projection showing an example of horizontal fracture of the neck of the condyle that is displaced laterally. (C) Open-mouth Towne projection showing an example of horizontal fracture of the neck of the condyle that is displaced medially. (D) Coronal section from a CBCT, showing bilateral vertical fractures of the condylar heads. (E) Coronal section from a CBCT, showing a vertical and medially displaced fracture of the left condylar head.
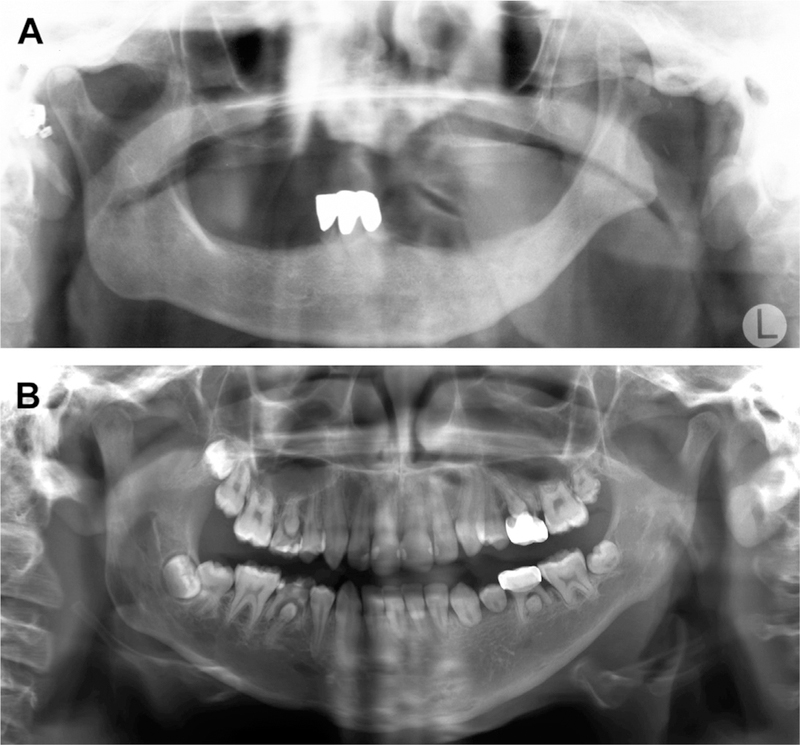
Aplasia or hypoplasia of the condyle. (A) An 85-year-old woman whose left condylar head and ramus are aplastic because of an osteomyelitis that had affected her left mandible when she was 10 years old. (B) Example of hypoplasia of the left condyle and ramus caused by childhood treatment with radiation therapy. Note multiple teeth with stunted roots as a result from the radiation therapy.
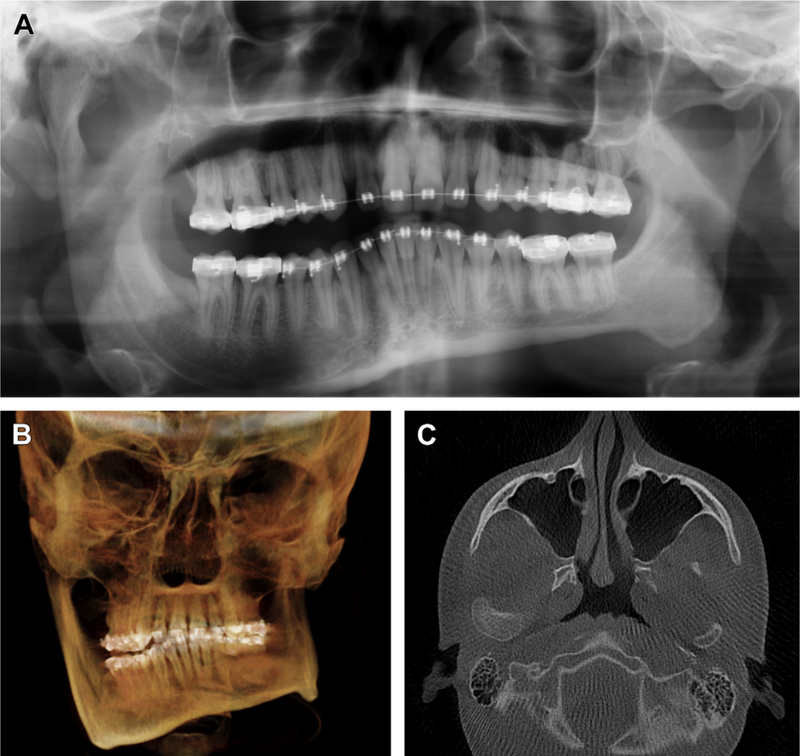
(A) Panoramic radiograph showing unilateral hyperplasia of the right condyle and right ramus. (B) Three-dimensional reconstruction of CBCT data of the same patient, showing significant facial asymmetry and right-sided posterior open bite. (C) Axial section of the same patient, showing significant hyperplasia of the right condyle in comparison with the left.
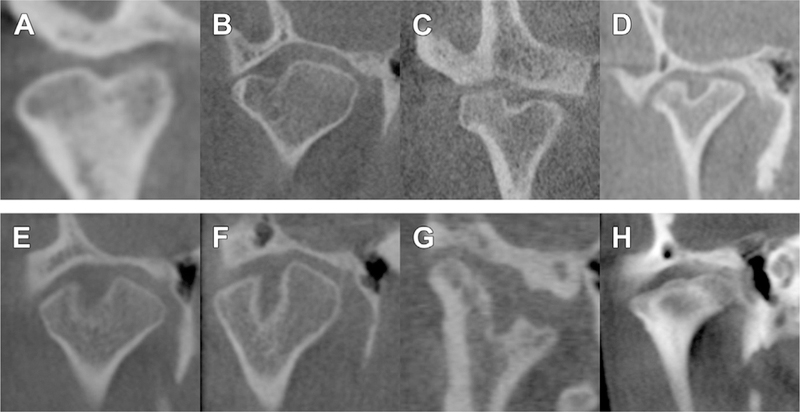
Axially corrected coronal views of condyles showing examples of bifidity. (A–G) Bifid condyles may have slight midline depression to almost a duplication of the condylar head. (H) Mild trifid appearance of the condylar head.
References
-
- Schiffman E, Ohrbach R, Truelove E, et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the International RDC/TMD Consortium Network* and orofacial pain special interest group†. J Oral Facial Pain Headache 2014;28(1):6–27. - PMC - PubMed
-
- Hunter A, Kalathingal S. Diagnostic imaging for temporomandibular disorders and orofacial pain. Dent Clin North Am 2013;57(3):405–18. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
