

The Role of Stereotactic Laser Amygdalohippocampotomy in Mesial Temporal Lobe Epilepsy
- PMID: 26615106
- PMCID: PMC5502117
- DOI: 10.1016/j.nec.2015.08.004
The Role of Stereotactic Laser Amygdalohippocampotomy in Mesial Temporal Lobe Epilepsy
Abstract
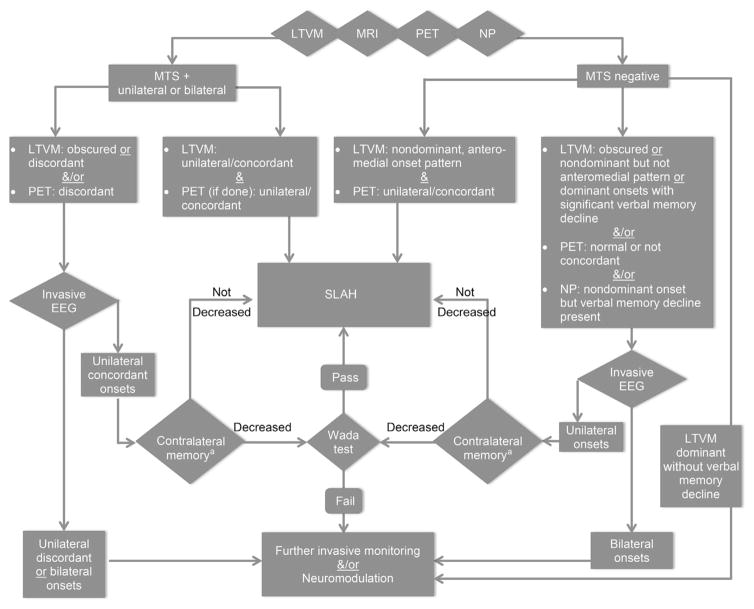
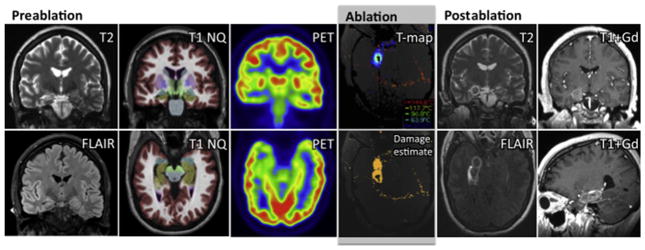
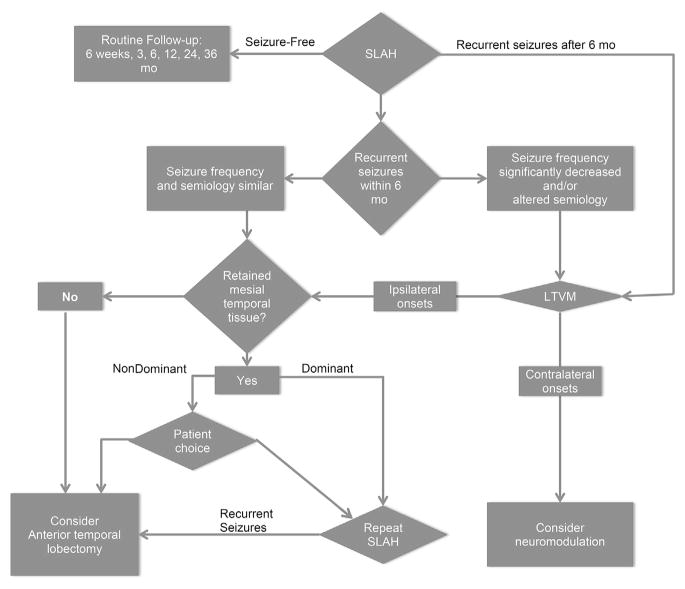
Stereotactic laser amygdalohippocampotomy (SLAH) uses laser interstitial thermal therapy guided by magnetic resonance thermography. This novel intervention can achieve seizure freedom while minimizing collateral damage compared to traditional open surgery, in patients with mesial temporal lobe epilepsy. An algorithm is presented to guide treatment decisions for initial and repeat procedures in patients with and without mesial temporal sclerosis. SLAH may improve access by medication-refractory patients to effective surgical treatments and thereby decrease medical complications, increase productivity, and minimize socioeconomic consequences in patients with chronic epilepsy.
Keywords: Ablation; Anterior temporal lobectomy; Laser; Memory; Mesial temporal lobe epilepsy; Mesial temporal sclerosis; Neuropsychology; Selective amygdalohippocampectomy.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
References
-
- Josephson CB, Dykeman J, Fiest KM, et al. Systematic review and meta-analysis of standard vs selective temporal lobe epilepsy surgery. Neurology. 2013;80(18):1669–76. - PubMed
-
- Mohammed HS, Kaufman CB, Limbrick DD, et al. Impact of epilepsy surgery on seizure control and quality of life: a 26-year follow-up study. Epilepsia. 2012;53(4):712–20. - PubMed
-
- Helmstaedter C. Cognitive outcomes of different surgical approaches in temporal lobe epilepsy. Epileptic Disord. 2013;15(3):221–39. - PubMed
-
- Baxendale S, Thompson PJ, Sander JW. Neuropsychological outcomes in epilepsy surgery patients with unilateral hippocampal sclerosis and good pre-operative memory function. Epilepsia. 2013;54(9):131–4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
