

Surgical complications following malignant brain tumor surgery: An analysis of 2002-2011 data
- PMID: 26615463
- PMCID: PMC4750489
- DOI: 10.1016/j.clineuro.2015.11.005
Surgical complications following malignant brain tumor surgery: An analysis of 2002-2011 data
Abstract
Objectives: To estimate the incidence of surgical complications and associated in-hospital morbidity and mortality following surgery for malignant brain tumors.
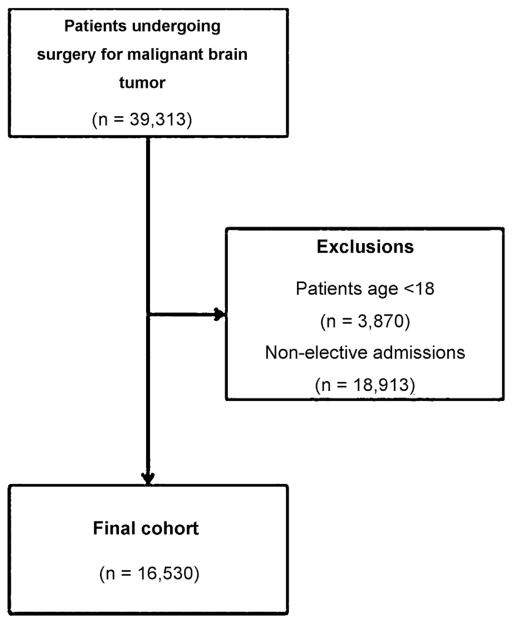
Patients and methods: The Nationwide Inpatient Sample (NIS) database was queried from 2002 to 2011. All adult patients who underwent elective brain surgery for a malignant brain tumor were included. Surgical complications included wrong side surgery, retention of a foreign object, iatrogenic stroke, meningitis, hemorrhage/hematoma complicating a procedure, and neurological complications. A regression model was conducted to estimate the odds ratios (OR) with their 95% confidence intervals (95% CI) of in-hospital mortality for each surgical complication.
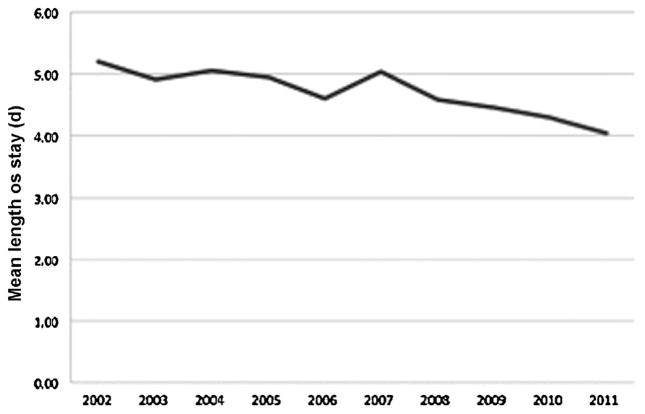
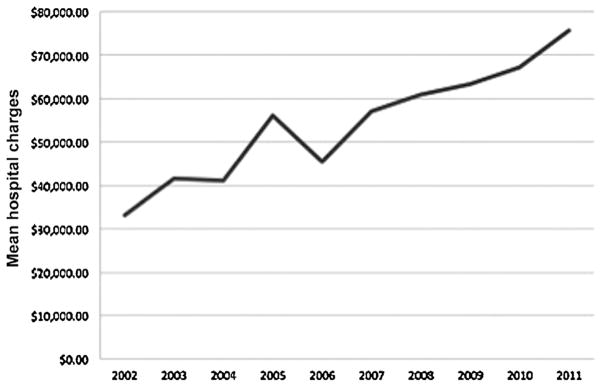
Results: A total of 16,530 admissions were analyzed, with 601 (36.2 events per 1000 cases) surgical complications occurring in 567 patients. Over the examined 10-year period, the overall incidence of surgical complications did not change (P=0.061) except for iatrogenic strokes, which increased in incidence from 14.1 to 19.8 events per 1000 between 2002 and 2011 (P=0.023). Patients who developed a surgical complication had significantly longer lengths of stay, total hospital costs, and higher rates of other complications. Patients who experienced an iatrogenic stroke had a significantly increased risk of mortality (OR 9.6; 95% 6.3-14.8) and so were patients with a hemorrhage/hematoma (OR 3.3; 95% CI 1.6-6.6).
Conclusion: In this study of an administrative database, patients undergoing surgery for a malignant brain tumor who suffered from a surgical complication had significantly longer lengths of stay, total hospital charges, and complication rates. Having a surgical complication was also an independent risk factor for in-hospital mortality. Nonetheless, it is unclear whether all surgical complications were clinically relevant, and further research is encouraged.
Keywords: Malignant brain tumor; Nationwide inpatient sample; Neurosurgery; Sentinel event; Surgical complication.
Copyright © 2015 Elsevier B.V. All rights reserved.
Conflict of interest statement
None.
Figures
References
-
- Omuro A, DeAngelis LM. Glioblastoma and other malignant gliomas: a clinical review. JAMA. 2013;310:1842–1850. - PubMed
-
- Sherman JH, Hoes K, Marcus J, Komotar RJ, Brennan CW, Gutin PH. Neurosurgery for brain tumors: update on recent technical advances. Curr Neurol Neurosci Rep. 2011;11:313–319. - PubMed
-
- Chaichana KL, Cabrera-Aldana EE, Jusue-Torres I, Wijesekera O, Olivi A, Rahman M, Quinones-Hinojosa A. When gross total resection of a glioblastoma is possible. How much resection should be achieved? World Neurosurg. 2014;82:257–265. - PubMed
-
- Chaichana KL, Jusue-Torres I, Navarro-Ramirez R, Raza SM, Pascual-Gallego M, Ibrahim A, Hernandez-Hermann M, Gomez L, Ye X, Weingart JD, Olivi A, Blakeley J, Gallia GL, Lim M, Brem H, Quinones-Hinojosa A. Establishing percent resection and residual volume thresholds affecting survival and recurrence for patients with newly diagnosed intracranial glioblastoma. Neuro-oncology. 2014;16:113–122. - PMC - PubMed
-
- Comission TJ. Sentinel Event. 2014;2014
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
