

Esmolol reduces anesthetic requirements thereby facilitating early extubation; a prospective controlled study in patients undergoing intracranial surgery
- PMID: 26615516
- PMCID: PMC4663038
- DOI: 10.1186/s12871-015-0154-1
Esmolol reduces anesthetic requirements thereby facilitating early extubation; a prospective controlled study in patients undergoing intracranial surgery
Abstract
Background: Adequate cerebral perfusion pressure with quick and smooth emergence from anesthesia is a major concern of the neuroanesthesiologist. Anesthesia techniques that minimize anesthetic requirements and their effects may be beneficial. Esmolol, a short acting hyperselective β-adrenergic blocker is effective in blunting adrenergic response to several perioperative stimuli and so it might interfere in the effect of the anesthetic drugs on the brain. This study was designed to investigate the effect of esmolol on the consumption of propofol and sevoflurane in patients undergoing craniotomy.
Method: Forty-two patients that underwent craniotomy for aneurysm clipping or tumour dissection were randomly divided in two groups (four subgroups). Anesthesia was induced with propofol, fentanyl and a single dose of cis-atracurium, followed by continuous infusion of remifentanil and either propofol or sevoflurane. Patients in the esmolol group received 500 mcg/kg of esmolol bolus 10 min before induction of anesthesia, followed by additional 200 mcg/kg/min of esmolol. Monitoring of the depth of anesthesia was also performed using the Bispectral Index-BIS and cardiac output. The inspired concentration of sevoflurane and the infusion rate of propofol were adjusted in order to maintain a BIS value between 40-50. Intraoperative emergence was detected by the elevation of BIS value, HR or MAP.
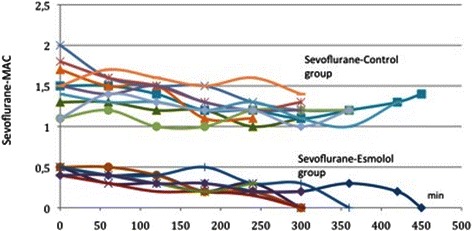
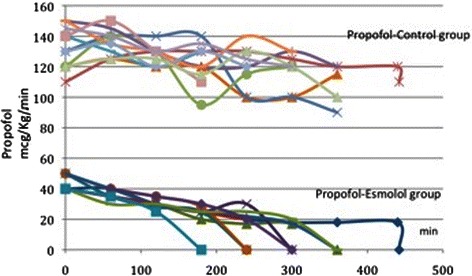
Results: The initial and the intraoperative doses of propofol and sevoflurane were 18-50 mcg/kg/min and 0.2-0.5 MAC respectively in the esmolol group, whereas in the control group they where 100-150 mcg/kg/ and 0.9-2.0 MAC respectively (p = 0.000 for both groups). All procedures were anesthesiologically uneventful with no episodes of intraoperative emerge.
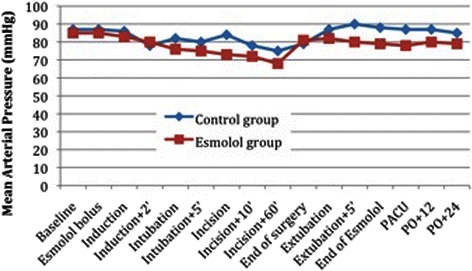
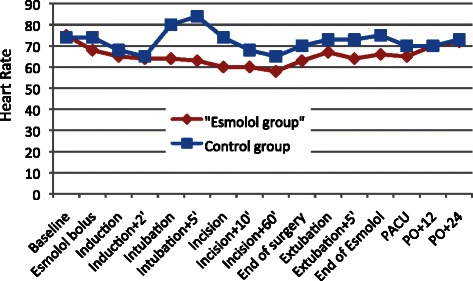
Conclusions: Esmolol is effective not only in attenuating intraoperative hemodynamic changes related to sympathetic overdrive but also in minimizing significant propofol and sevoflurane requirements without compromising the hemodynamic status. ClinicalTrials.gov Identifier: NCT02455440 . Registered 26 May 2015.
Figures
References
-
- Bruder N, Stordeur JM, Ravussin P, Valli M, Dufour H, Bruguerolle B, et al. Metabolic and hemodynamic changes during recovery and tracheal extubation in neurosurgical patients: immediate versus delayed recovery. Anesth Analg. 1999;89:674–8. - PubMed
-
- Hans P, Bonhomme V. Why we still use intravenous drugs as the basic regimen for neurosurgical anaesthesia. Curr Opin Anaesthesiol. 2006;19:498–503. doi: 10.1097/01.aco.0000245274.69292.ad. - DOI - PubMed
-
- Bilotta F, Doronzio A, Cuzzone V, Caramia R, Rosa G. Early postoperative cognitive recovery and gas exchange patterns after balanced anesthesia with sevoflurane or desflurane in overweight and obese patients undergoing craniotomies. J Neurosurg Anesthesiol. 2009;21:207–13. doi: 10.1097/ANA.0b013e3181a19c52. - DOI - PubMed
-
- Fraga M, Rama-Maceiras P, Rodiño S, Aymerich H, Pose P, Belda J. The effects of isoflurane and desflurane on intracranial pressure, cerebral perfusion pressure, and cerebral arteriovenous oxygen content difference in normocapnic patients with supratentorial brain tumors. Anesthesiology. 2003;98:1085–90. doi: 10.1097/00000542-200305000-00010. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
