

Horizontal Inequity in Elderly Health Care Utilization: Evidence from India
- PMID: 26617450
- PMCID: PMC4659869
- DOI: 10.3346/jkms.2015.30.S2.S155
Horizontal Inequity in Elderly Health Care Utilization: Evidence from India
Abstract
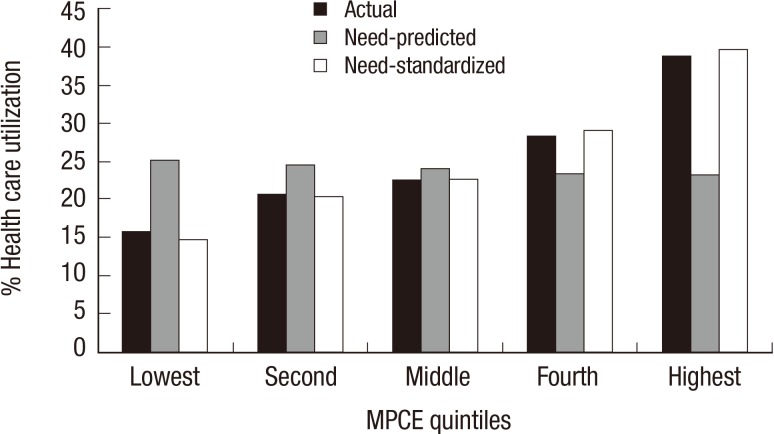
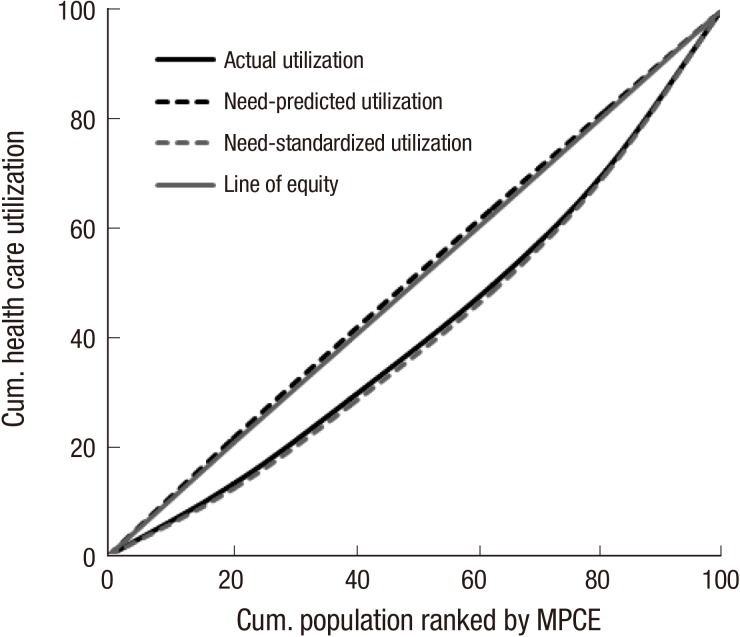
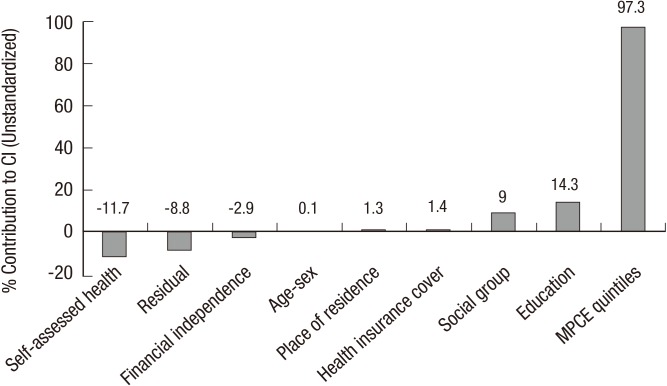
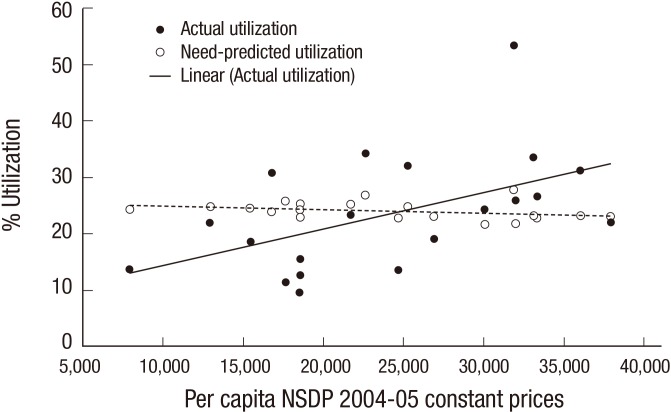
Against the backdrop of population aging, this paper presents the analysis of need-standardised health care utilization among elderly in India. Based on nationally representative morbidity and health care survey 2004, we demonstrate that the need for health care utilization is indeed pro-poor in nature. However, the actual health care utilization is concentrated among richer sections of the population. Further, the decomposition analysis reveals that income has a very strong role in shifting the distribution of health care away from the poor elderly. The impact of income on utilization is well-demonstrated even at the ecological-level as states with higher per capita incomes have higher elderly health care utilization even as the levels of need-predicted distribution across these states are similar. We also find that the distribution of elderly across social groups and their educational achievements favours the rich and significantly contributes to overall inequality. Nevertheless, contribution of need-related self-assessed health clearly favours pro-poor inequality. In concluding, we argue that to reduce such inequities in health care utilization it is necessary to increase public investments in health care infrastructure including geriatric care particularly in rural areas and underdeveloped regions to enhance access and quality of health care for the elderly.
Keywords: Aged; Delivery of Health Care; Health Care; Socioeconomic Factors; Surveys.
Figures

References
-
- United Nations. World population ageing 2013. ST/ESA/SER.A/348. New York: Department of Economic and Social Affairs, Population Division; 2013.
-
- Giridhar G, Sathyanarayana K, Kumar S, James K, Alam M. Population ageing in India. Delhi: Cambridge University Press; 2014.
-
- National Sample Survey Organisation. Morbidity health care and the condition of aged: report no 507. New Delhi: Ministry of Statistics and Programme Implementation; 2006.
-
- Wagstaff A, van Doorslaer E. Equity in health care finance and delivery. In: Culyer AJ, Newhouse JP, editors. Handbook of Health Economics (1B) Amsterdam: Elsevier; 2000. pp. 1803–1862.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
