

Integrated genomic characterization of IDH1-mutant glioma malignant progression
- PMID: 26618343
- PMCID: PMC4829945
- DOI: 10.1038/ng.3457
Integrated genomic characterization of IDH1-mutant glioma malignant progression
Abstract
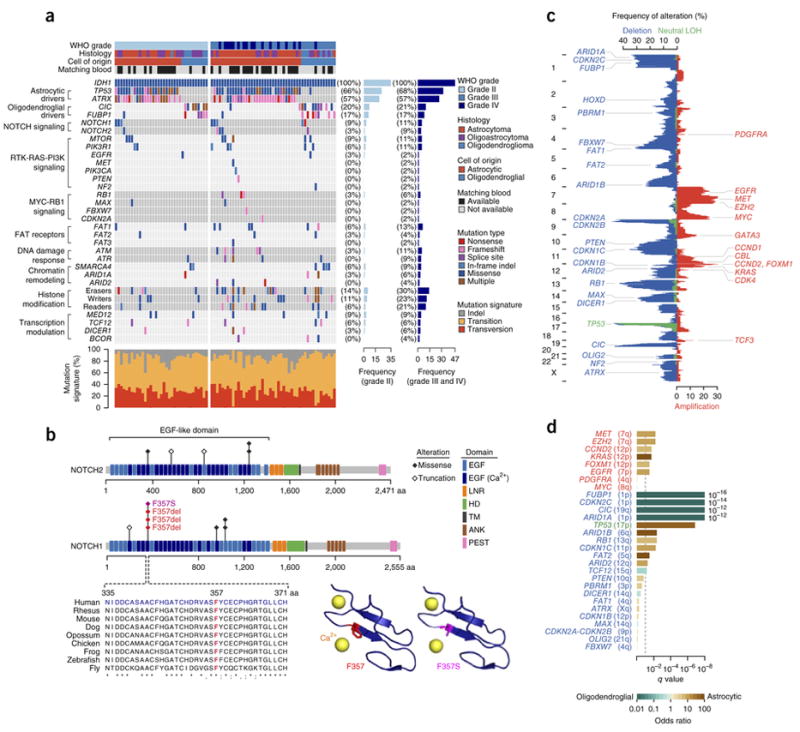
Gliomas represent approximately 30% of all central nervous system tumors and 80% of malignant brain tumors. To understand the molecular mechanisms underlying the malignant progression of low-grade gliomas with mutations in IDH1 (encoding isocitrate dehydrogenase 1), we studied paired tumor samples from 41 patients, comparing higher-grade, progressed samples to their lower-grade counterparts. Integrated genomic analyses, including whole-exome sequencing and copy number, gene expression and DNA methylation profiling, demonstrated nonlinear clonal expansion of the original tumors and identified oncogenic pathways driving progression. These include activation of the MYC and RTK-RAS-PI3K pathways and upregulation of the FOXM1- and E2F2-mediated cell cycle transitions, as well as epigenetic silencing of developmental transcription factor genes bound by Polycomb repressive complex 2 in human embryonic stem cells. Our results not only provide mechanistic insight into the genetic and epigenetic mechanisms driving glioma progression but also identify inhibition of the bromodomain and extraterminal (BET) family as a potential therapeutic approach.
Conflict of interest statement
The authors declare competing financial interests: details are available in the online version of the paper.
Figures





References
-
- Claus EB, Black PM. Survival rates and patterns of care for patients diagnosed with supratentorial low-grade gliomas. Cancer. 2006;106:1358–1363. - PubMed
-
- Stupp R, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352:987–996. - PubMed
-
- Stupp R, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–466. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
