

Airway CD8(+) T Cells Are Associated with Lung Injury during Infant Viral Respiratory Tract Infection
- PMID: 26618559
- PMCID: PMC4942220
- DOI: 10.1165/rcmb.2015-0297OC
Airway CD8(+) T Cells Are Associated with Lung Injury during Infant Viral Respiratory Tract Infection
Abstract
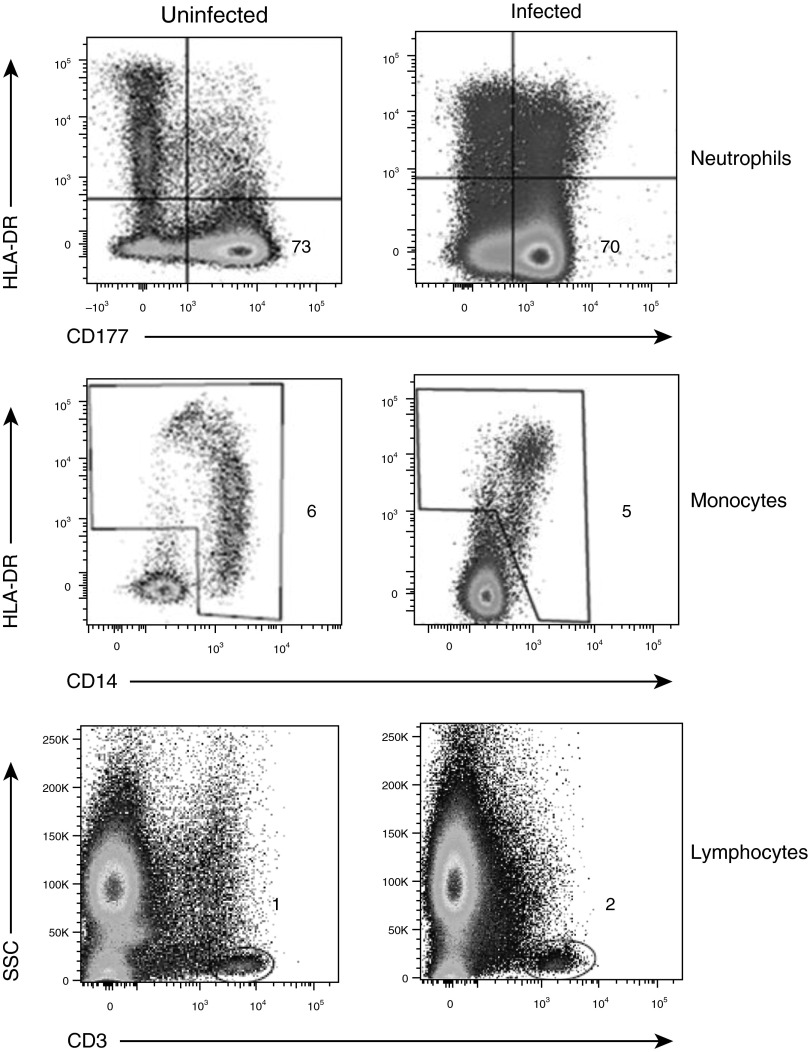
Infants and young children are disproportionately susceptible to severe complications from respiratory viruses, although the underlying mechanisms remain unknown. Recent studies show that the T cell response in the lung is important for protective responses to respiratory infections, although details on the infant/pediatric respiratory immune response remain sparse. The objectives of the present study were to characterize the local versus systemic immune response in infants and young children with respiratory failure from viral respiratory tract infections and its association to disease severity. Daily airway secretions were sampled from infants and children 4 years of age and younger receiving mechanical ventilation owing to respiratory failure from viral infection or noninfectious causes. Samples were examined for immune cell composition and markers of T cell activation. These parameters were then correlated with clinical disease severity. Innate immune cells and total CD3(+) T cells were present in similar proportions in airway aspirates derived from infected and uninfected groups; however, the CD8:CD4 T cell ratio was markedly increased in the airways of patients with viral infection compared with uninfected patients, and specifically in infected infants with acute lung injury. T cells in the airways were phenotypically and functionally distinct from those in blood with activated/memory phenotypes and increased cytotoxic capacity. We identified a significant increase in airway cytotoxic CD8(+) T cells in infants with lung injury from viral respiratory tract infection that was distinct from the T cell profile in circulation and associated with increasing disease severity. Airway sampling could therefore be diagnostically informative for assessing immune responses and lung damage.
Keywords: immunopathology; infant immunity; lung injury; viral pneumonia.
Figures






References
-
- Spaeder MC, Custer JW, Bembea MM, Aganga DO, Song X, Scafidi S. A multicenter outcomes analysis of children with severe viral respiratory infection due to human metapneumovirus. Pediatr Crit Care Med. 2013;14:268–272. - PubMed
-
- Levy O. Innate immunity of the newborn: basic mechanisms and clinical correlates. Nat Rev Immunol. 2007;7:379–390. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
