

Pan-cancer analysis of the extent and consequences of intratumor heterogeneity
- PMID: 26618723
- PMCID: PMC4830693
- DOI: 10.1038/nm.3984
Pan-cancer analysis of the extent and consequences of intratumor heterogeneity
Abstract
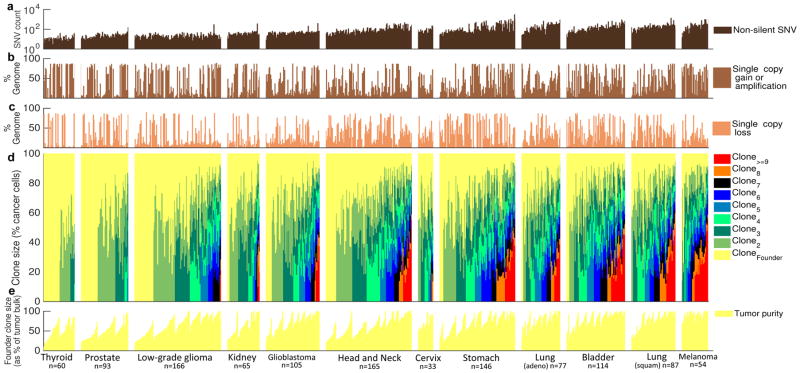
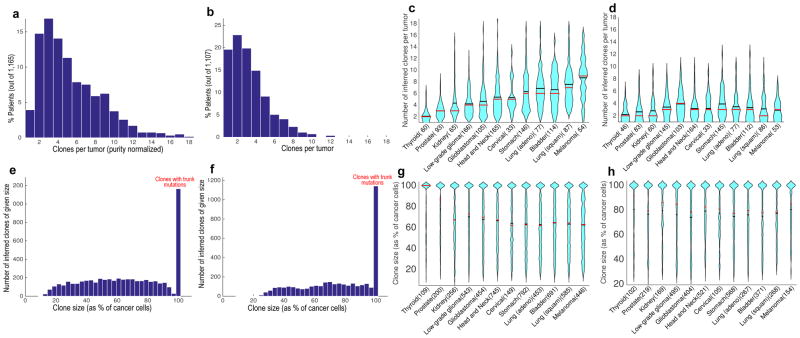
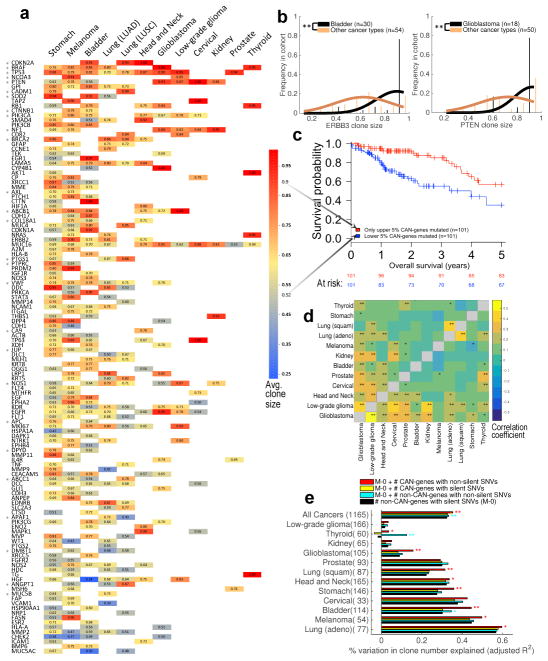
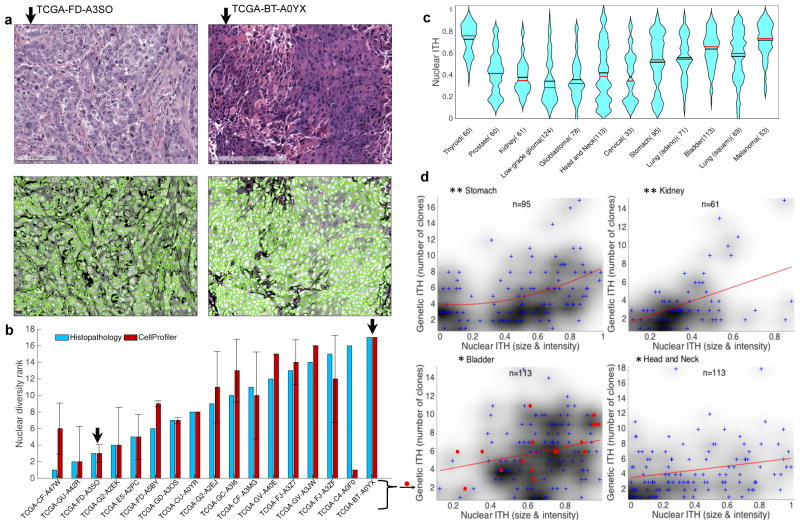
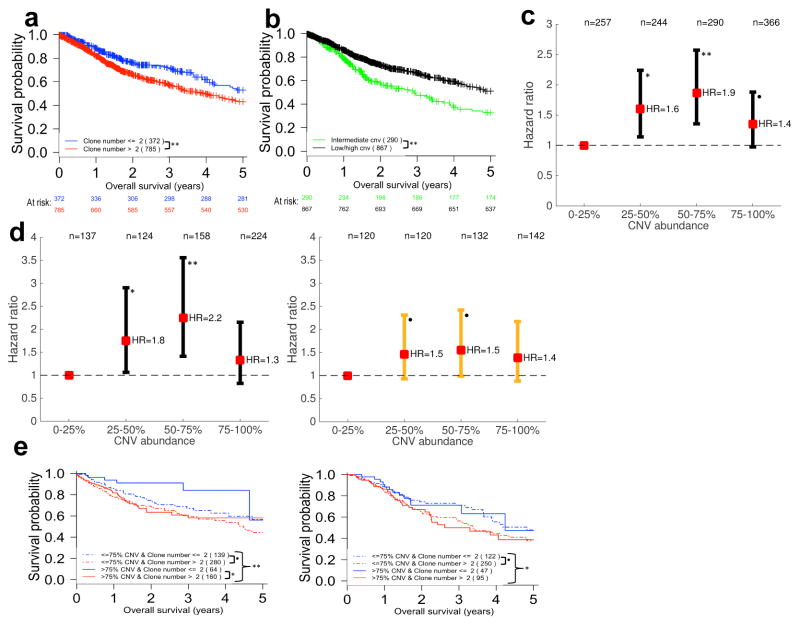
Intratumor heterogeneity (ITH) drives neoplastic progression and therapeutic resistance. We used the bioinformatics tools 'expanding ploidy and allele frequency on nested subpopulations' (EXPANDS) and PyClone to detect clones that are present at a ≥10% frequency in 1,165 exome sequences from tumors in The Cancer Genome Atlas. 86% of tumors across 12 cancer types had at least two clones. ITH in the morphology of nuclei was associated with genetic ITH (Spearman's correlation coefficient, ρ = 0.24-0.41; P < 0.001). Mutation of a driver gene that typically appears in smaller clones was a survival risk factor (hazard ratio (HR) = 2.15, 95% confidence interval (CI): 1.71-2.69). The risk of mortality also increased when >2 clones coexisted in the same tumor sample (HR = 1.49, 95% CI: 1.20-1.87). In two independent data sets, copy-number alterations affecting either <25% or >75% of a tumor's genome predicted reduced risk (HR = 0.15, 95% CI: 0.08-0.29). Mortality risk also declined when >4 clones coexisted in the sample, suggesting a trade-off between the costs and benefits of genomic instability. ITH and genomic instability thus have the potential to be useful measures that can universally be applied to all cancers.
Conflict of interest statement
The authors declare no competing financial interests.
Figures
Comment in
-
Genetics: Intratumour heterogeneity - a game of snakes and ladders.Nat Rev Clin Oncol. 2016 Jan;13(1):1. doi: 10.1038/nrclinonc.2015.219. Epub 2015 Dec 15. Nat Rev Clin Oncol. 2016. PMID: 26667972 No abstract available.
References
-
- Nowell PC. The clonal evolution of tumor cell populations. Science. 1976;194:23–28. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 HG006137/HG/NHGRI NIH HHS/United States
- U01 CA176299/CA/NCI NIH HHS/United States
- R01 CA185138/CA/NCI NIH HHS/United States
- R01 NS080619/NS/NINDS NIH HHS/United States
- P01 HG000205/HG/NHGRI NIH HHS/United States
- P01 CA091955/CA/NCI NIH HHS/United States
- R01 CA149566/CA/NCI NIH HHS/United States
- R01 CA164746/CA/NCI NIH HHS/United States
- R01 CA170595/CA/NCI NIH HHS/United States
- U01CA17629901/CA/NCI NIH HHS/United States
- Howard Hughes Medical Institute/United States
- U01CA151920/CA/NCI NIH HHS/United States
- R01 NS08061904/NS/NINDS NIH HHS/United States
- P01 CA91955/CA/NCI NIH HHS/United States
- R01 CA140657/CA/NCI NIH HHS/United States
- U01 CA151920/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
