

Does Surgical Approach Affect Patient-reported Function After Primary THA?
- PMID: 26620966
- PMCID: PMC4773324
- DOI: 10.1007/s11999-015-4639-5
Does Surgical Approach Affect Patient-reported Function After Primary THA?
Abstract
Background: Total hip arthroplasty (THA) relieves pain and improves physical function in patients with hip osteoarthritis, but requires a year or more for full postoperative recovery. Proponents of intermuscular surgical approaches believe that the direct-anterior approach may restore physical function more quickly than transgluteal approaches, perhaps because of diminished muscle trauma. To evaluate this, we compared patient-reported physical function and other outcome metrics during the first year after surgery between groups of patients who underwent primary THA either through the direct-anterior approach or posterior approach.
Questions/purposes: We asked: (1) Is a primary THA using a direct-anterior approach associated with better patient-reported physical function at early postoperative times (1 and 3 months) compared with a THA performed through the posterior approach? (2) Is the direct-anterior approach THA associated with shorter operative times and higher rates of noninstitutional discharge than a posterior approach THA?
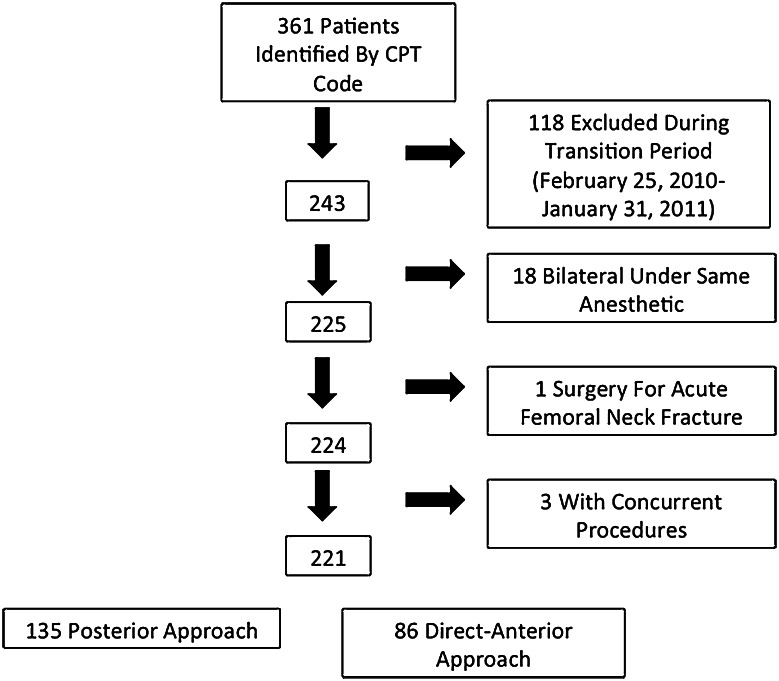
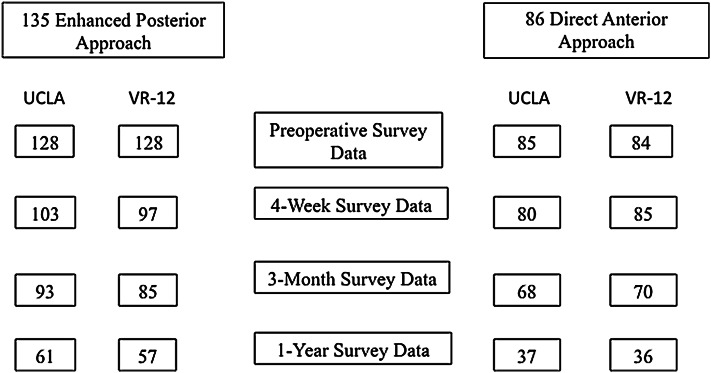
Methods: Between October 2008 and February 2010, an arthroplasty fellowship-trained surgeon performed 135 THAs. All 135 were performed using the posterior approach. During that period, we used this approach when patients had any moderate to severe degenerative joint disease of the hip attributable to any type of arthritis refractory to nonoperative treatment measures. Of the patients who were treated with this approach, 21 (17%; 23 hips) were lost to followup, whereas 109 (83%; 112 hips) were available for followup at 1 year. Between February and September 2011, the same surgeon performed 86 THAs. All 86 were performed using the direct-anterior approach. During that period, we used this approach when patients with all types of moderate to severe degenerative joint disease had nonoperative treatment measures fail. Of the patients who were treated with this approach, 35 (41%; 35 hips) were lost to followup, whereas 51 (59%; 51 hips) were available for followup at 1 year. THAs during the surgeon's direct-anterior approach learning period (February 2010 through January 2011) were excluded because both approaches were being used selectively depending on patient characteristics. Clinical outcomes included operative blood loss; allogeneic transfusion; adverse events; patient-reported Veterans RAND-12 Physical (PCS) and Mental Component Summary (MCS) scores, and University of California Los Angeles (UCLA) activity scores at 1 month, 3 months, and 1 year after surgery. Resource utilization outcomes included operative time, length of stay, and discharge disposition (home versus institution). Outcomes were compared using logistic and linear regression techniques.
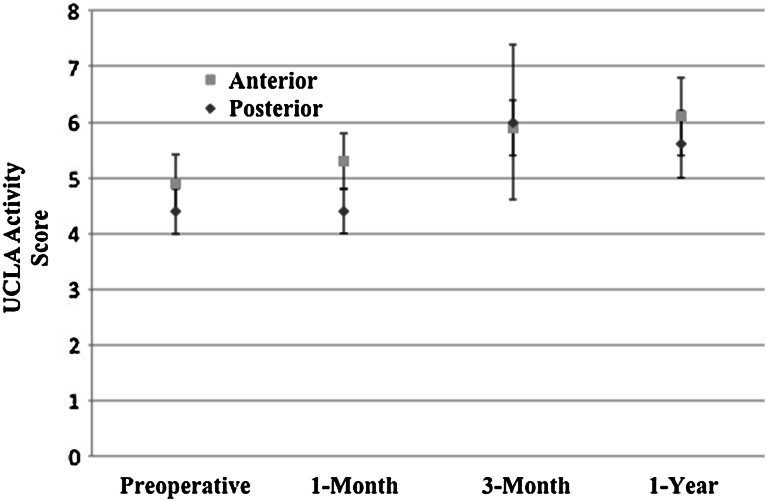
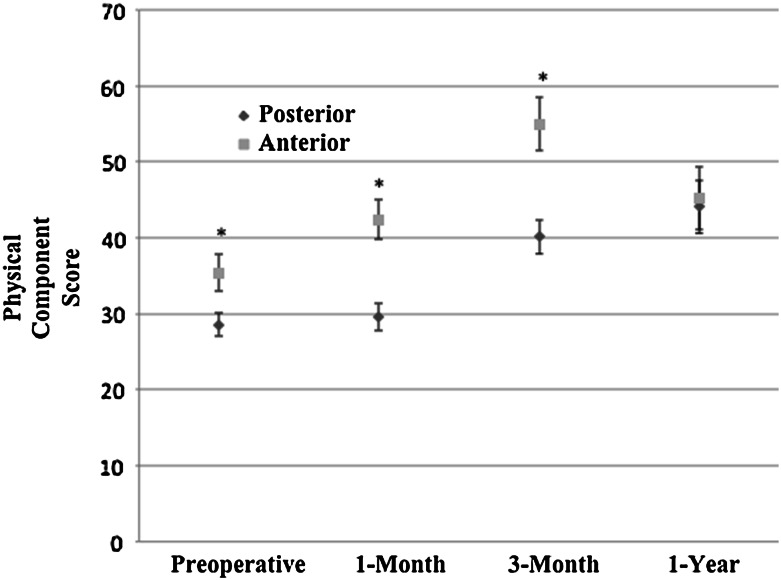
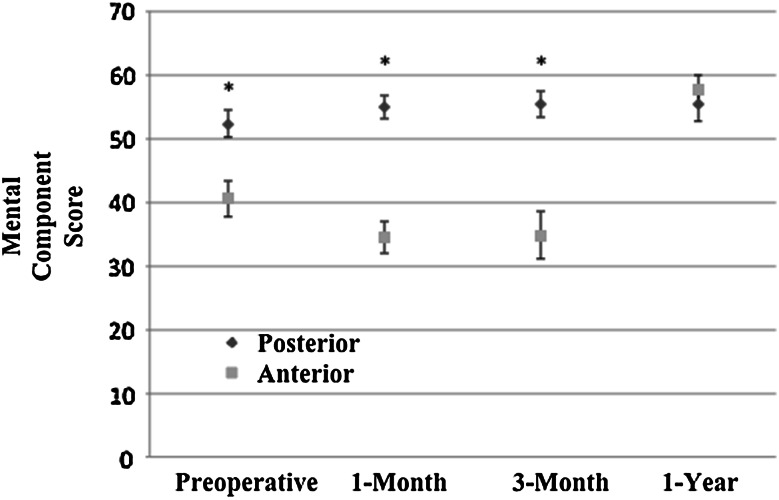
Results: After controlling for relevant confounding variables including age, sex, and BMI, the direct-anterior approach was associated with worse adjusted MCS changes 1 and 3 months after surgery (1-month score change, -9; 95% CI, -13 to -5; standard error, 2), compared with the posterior approach (3-month score change, -9; 95% CI, -14 to -3; standard error, 3) (both p < 0.001), while the direct-anterior approach was associated with greater PCS improvement at 3 months compared with the posterior approach (score change, 6; 95% CI, 2-10; standard error, 2; p = 0.008). There were no differences in adjusted PCS at either 1 month or 12 months, and no clinically important differences in UCLA scores. Although the PCS score differences are greater than the minimum clinically important difference of 5 points for this endpoint, the clinical importance of such a small effect is questionable. At 1 year after THA, there were no intergroup differences in self-reported physical function, although both groups had significant loss-to-followup at that time. Operative time (skin incision to skin closure) between the two groups did not differ (81 versus 79 minutes; p = 0.411). Mean surgical blood loss (403 versus 293 mL; p < 0.001; adjusted, 119 more mL; 95% CI, 79-160; p < 0.001) and in-hospital transfusion rates (direct-anterior approach, 20% [17/86] versus posterior approach, 10% [14/135], p = 0.050; adjusted odds ratio, 3.6; 95% CI, 1.3-10.1; p = 0.016) were higher in the direct-anterior approach group. With the numbers available, there was no difference in the frequency of adverse events between groups when comparing intraoperative complications, perioperative Technical Expert Panel complications, and other non-Technical Expert Panel complications within 1 year of surgery, although this study was not adequately powered to detect differences in rare adverse events.
Conclusions: With suitable experience, the direct-anterior approach can be performed with expected results similar to those of the posterior approach. There may be transient and small benefits to the direct-anterior approach, including improved physical function at 3 months after surgery. However, the greater operative blood loss and greater likelihood of blood transfusions, even when the surgeon is experienced, may be a disadvantage. Given some of the kinds of bias present that we found, including loss to followup, the conclusions we present should be considered preliminary, but it appears that any benefits that accrue to the patients who had the direct-anterior approach would be transient and modest. Prospective randomized studies on the topic are needed to address the differences between surgical approaches more definitively.
Level of evidence: Level III, therapeutic study.
Figures
Comment in
-
CORR Insights®: Does Surgical Approach Affect Patient-reported Function After Primary THA?Clin Orthop Relat Res. 2016 Apr;474(4):982-4. doi: 10.1007/s11999-015-4685-z. Epub 2016 Jan 4. Clin Orthop Relat Res. 2016. PMID: 26728520 Free PMC article. No abstract available.
References
-
- Bergin PF, Doppelt JD, Kephart CJ, Benke MT, Graeter JH, Holmes AS, Haleem-Smith H, Tuan RS, Unger AS. Comparison of minimally invasive direct anterior versus posterior total hip arthroplasty based on inflammation and muscle damage markers. J Bone Joint Surg Am. 2011;93:1392–1398. doi: 10.2106/JBJS.J.00557. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
