

Chronic mucocutaneous candidiasis: characterization of a family with STAT-1 gain-of-function and development of an ex-vivo assay for Th17 deficiency of diagnostic utility
- PMID: 26621323
- PMCID: PMC4837241
- DOI: 10.1111/cei.12746
Chronic mucocutaneous candidiasis: characterization of a family with STAT-1 gain-of-function and development of an ex-vivo assay for Th17 deficiency of diagnostic utility
Abstract
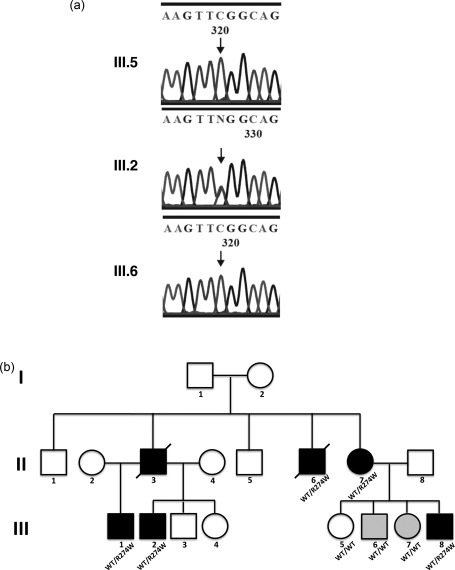
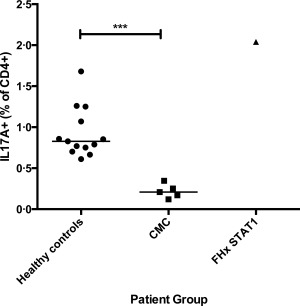
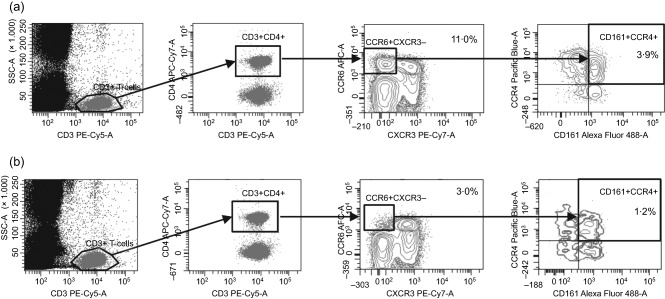
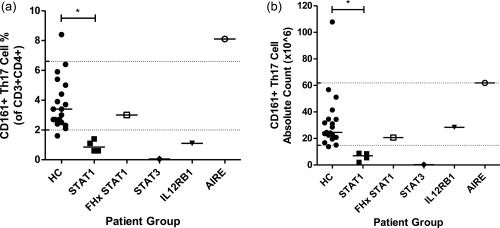
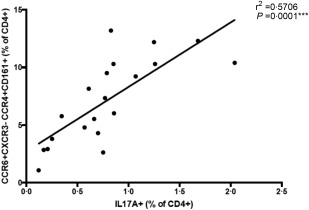
Chronic mucocutaneous candidiasis (CMC) is characterized by recurrent and persistent superficial infections, with Candida albicans affecting the mucous membranes, skin and nails. It can be acquired or caused by primary immune deficiencies, particularly those that impair interleukin (IL)-17 and IL-22 immunity. We describe a single kindred with CMC and the identification of a STAT1 GOF mutation by whole exome sequencing (WES). We show how detailed clinical and immunological phenotyping of this family in the context of WES has enabled revision of disease status and clinical management. Together with analysis of other CMC cases within our cohort of patients, we used knowledge arising from the characterization of this family to develop a rapid ex-vivo screening assay for the detection of T helper type 17 (Th17) deficiency better suited to the routine diagnostic setting than established in-vitro techniques, such as intracellular cytokine staining and enzyme-linked immunosorbent assay (ELISA) using cell culture supernatants. We demonstrate that cell surface staining of unstimulated whole blood for CCR6⁺ CXCR3⁻ CCR4⁺ CD161⁺ T helper cells generates results that correlate with intracellular cytokine staining for IL-17A, and is able to discriminate between patients with molecularly defined CMC and healthy controls with 100% sensitivity and specificity within the cohort tested. Furthermore, removal of CCR4 and CD161 from the antibody staining panel did not affect assay performance, suggesting that the enumeration of CCR6⁺ CXCR3⁻ CD4⁺ T cells is sufficient for screening for Th17 deficiency in patients with CMC and could be used to guide further investigation aimed at identifying the underlying molecular cause.
Keywords: Th17; chemokine receptors; chronic mucocutaneous candidiasis; surface phenotyping.
© 2016 The Authors. Clinical & Experimental Immunology published by John Wiley & Sons Ltd on behalf of British Society for Immunology.
Figures
References
-
- Lilic D. Unravelling fungal immunity through primary immune deficiencies. Curr Opin Microbiol 2012; 15:420–6. - PubMed
-
- Engelhardt KR, Grimbacher B. Mendelian traits causing susceptibility to mucocutaneous fungal infections in human subjects. J Allergy Clin Immunol 2012; 129:294–305; quiz 6–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
