

The Association of Brain MRI Characteristics and Postoperative Delirium in Cardiac Surgery Patients
- PMID: 26621626
- PMCID: PMC5384473
- DOI: 10.1016/j.clinthera.2015.10.021
The Association of Brain MRI Characteristics and Postoperative Delirium in Cardiac Surgery Patients
Abstract
Purpose: Delirium is common after cardiac surgery and is associated with adverse consequences, including cognitive decline. Identification of vulnerable older adults might allow for early implementation of delirium-prevention strategies. Brain MRI findings provide insight into structural brain changes that may identify vulnerable patients. The purpose of this study was to examine the association between brain MRI characteristics potentially associated with delirium vulnerability and the development of postoperative delirium in a nested cohort of patients undergoing cardiac surgery.
Methods: We identified 79 cardiac surgery patients who had brain MRI imaging after cardiac surgery, as part of an ongoing randomized trial evaluating the efficacy of blood pressure management based on cerebral autoregulation monitoring versus standard management for improving neurological outcomes. Cerebral lateral ventricular size, cortical sulcal width, and white matter hyperintensities (WMH) on brain MRI scans were graded on a validated 0 to 9 scale, and categorized into tertiles. New ischemic lesions were characterized as present or absent. Delirium was assessed using a validated chart-review. Neuropsychological testing performed before surgery was used to establish preoperative cognitive baseline. Multivariable logistic regression was used to assess the independent association between MRI characteristics and postoperative delirium.
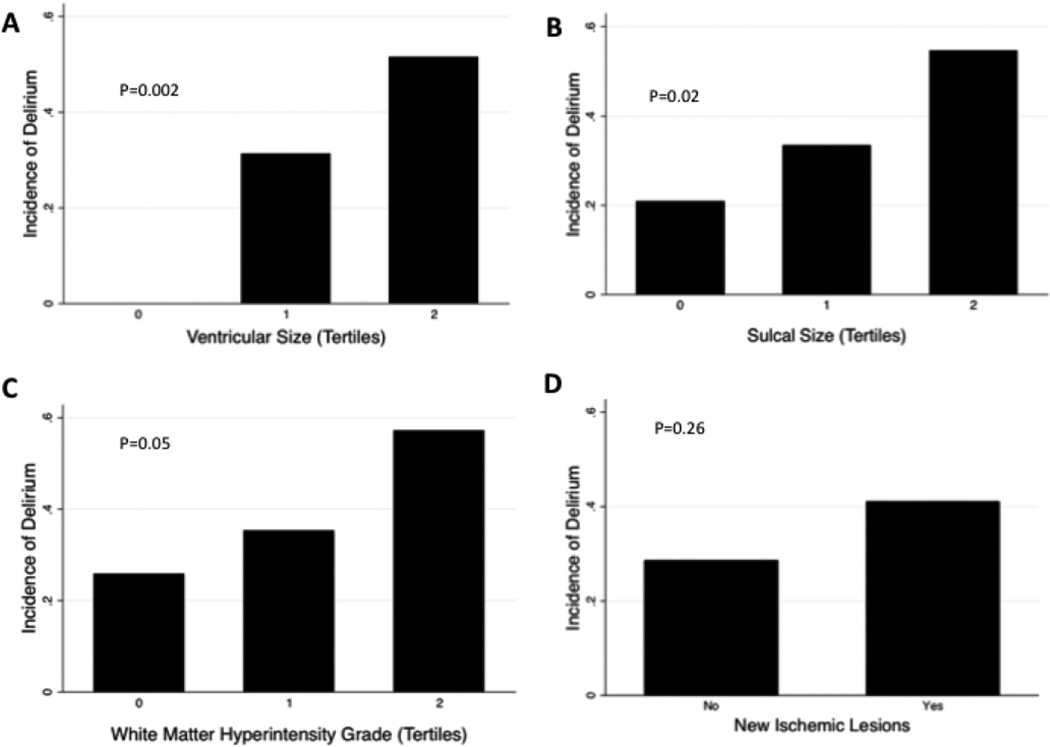
Findings: The average age of patients was 70.1 ± 7.8 years old, and 72% were male. Twenty-eight of 79 (35.4%) patients developed postoperative delirium. Patients with delirium had higher unadjusted ventricular size (median 4 vs. 3, P = 0.003), and there was a trend towards higher sulcal sizes and WMH grades. Increasing tertiles of ventricular size (Odds Ratio [OR] 3.59; 95% Confidence Interval [CI] 1.59-8.12; P = 0.002) and sulcal size (OR 2.15; 95%CI 1.13-4.12; P = 0.02) were associated with postoperative delirium, with a trend for tertiles of WMH grade (OR 1.91; 95%CI 0.99-3.68; P = 0.05). In multivariable models adjusted for logistic EuroSCORE, baseline cognitive status, bypass time, and any postoperative complication, each tertile of ventricular size was associated with increased odds of postoperative delirium (OR 3.23 per tertile increase in ventricular size; 95%CI 1.21-8.60; P = 0.02). There were no differences in odds of delirium by tertiles of sulcal grade, tertiles of white matter grade, or presence of new ischemic lesions, in adjusted models.
Implications: Increased brain ventricular size was independently associated with delirium after cardiac surgery. These results suggest that cerebral atrophy may contribute to increased vulnerability for postoperative delirium. Baseline brain MRIs may be useful in identifying cardiac surgery patients at high risk for postoperative delirium, who might benefit from targeted perioperative approaches to prevent delirium. ClinicalTrials.gov identifier: NCT00981474.
Keywords: cardiac surgery; postoperative delirium; sulcal width; ventricular size; white matter hyperintensities.
Copyright © 2015 Elsevier HS Journals, Inc. All rights reserved.
Conflict of interest statement
There are no conflicts of interest. For unrelated studies, Karin Neufeld has received research support from Ornim Medical, and Charles Hogue has received research support from Covidien, Inc. and served on the advisory board for Ornim Medical.
Figures
References
-
- Ottens TH, Dieleman JM, Sauër A-MC, et al. Effects of dexamethasone on cognitive decline after cardiac surgery: a randomized clinical trial. Anesthesiology. 2014;121(3):492–500. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
