

Right heart catheterisation: best practice and pitfalls in pulmonary hypertension
- PMID: 26621978
- PMCID: PMC9487613
- DOI: 10.1183/16000617.0062-2015
Right heart catheterisation: best practice and pitfalls in pulmonary hypertension
Abstract
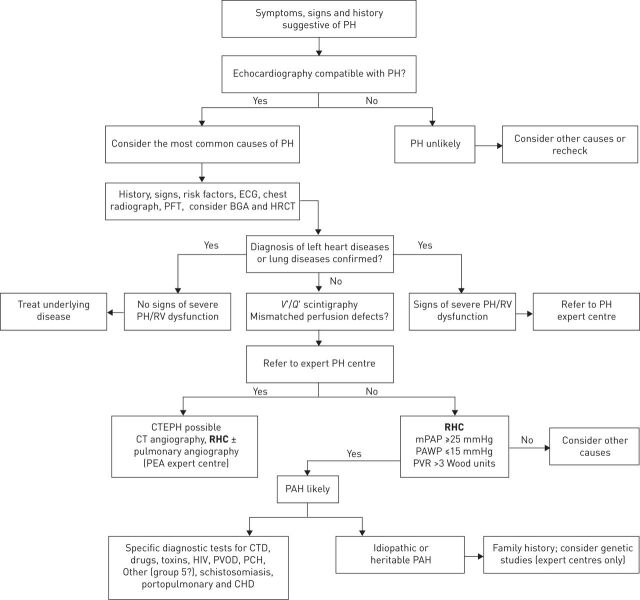
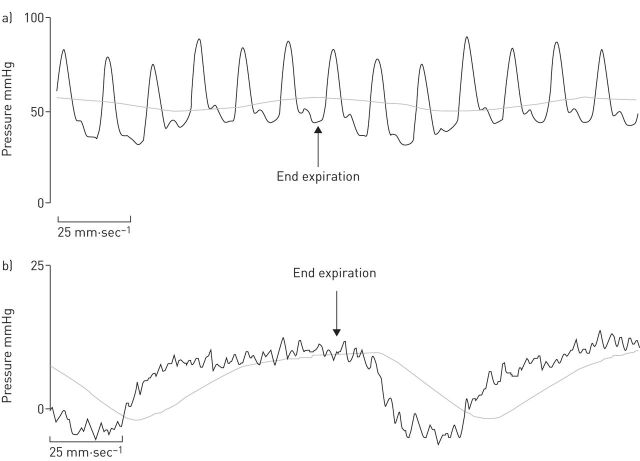
Right heart catheterisation (RHC) plays a central role in identifying pulmonary hypertension (PH) disorders, and is required to definitively diagnose pulmonary arterial hypertension (PAH). Despite widespread acceptance, there is a lack of guidance regarding the best practice for performing RHC in clinical practice. In order to ensure the correct evaluation of haemodynamic parameters directly measured or calculated from RHC, attention should be drawn to standardising procedures such as the position of the pressure transducer and catheter balloon inflation volume. Measurement of pulmonary arterial wedge pressure, in particular, is vulnerable to over- or under-wedging, which can give rise to false readings. In turn, errors in RHC measurement and data interpretation can complicate the differentiation of PAH from other PH disorders and lead to misdiagnosis. In addition to diagnosis, the role of RHC in conjunction with noninvasive tests is widening rapidly to encompass monitoring of treatment response and establishing prognosis of patients diagnosed with PAH. However, further standardisation of RHC is warranted to ensure optimal use in routine clinical practice.
Copyright ©ERS 2015.
Conflict of interest statement
Conflict of interest: Disclosures can be found alongside the online version of this article at
Figures

References
-
- Chatterjee K. The Swan-Ganz catheters: past, present, and future. A viewpoint. Circulation 2009; 119: 147–152. - PubMed
-
- Hoeper MM, Bogaard HJ, Condliffe R, et al. . Definitions and diagnosis of pulmonary hypertension. J Am Coll Cardiol 2013; 62: Suppl., D42–D50. - PubMed
-
- Galiè N, Humbert M, Vachiery JL, et al. . 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J 2015; 46: 903–975. - PubMed
-
- Simonneau G, Gatzoulis MA, Adatia I, et al. . Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol 2013; 62: Suppl., D34–D41. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical